Nonsteroidal Anti-inflammatory Drugs
Nonsteroidal anti-inflammatory drugs (NSAIDs) work by blocking inflammation at the site of pathology and by altering pain perception in the central nervous system (CNS). Peripherally, cyclooxygenase is an enzyme that converts arachidonic acid to a number of prostaglandins. Hormone-like substances, prostaglandins, participate in a wide range of body functions such as cell growth and the dilatation and constriction of blood vessels, as well as inflammation. The inflammatory prostaglandins sensitize nerve endings to the action of bradykinin, histamine, and other inflammatory factors, making them more likely to transmit pain. Peripherally, NSAIDs block the action of cyclooxygenase, halting the conversion of arachidonic acid into inflammatory prostaglandins, the key step in the inflammatory cascade (Fig. 9-1).
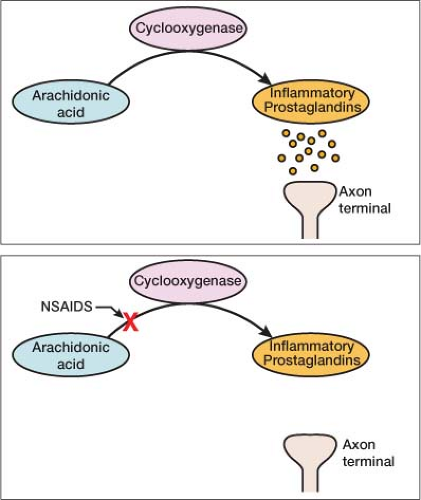 Figure 9-1 Cyclooxygenase, the enzyme blocked by NSAIDs, converts arachidonic acid to inflammatory prostaglandins. |
The cyclooxygenase enzyme has two isoforms: COX-1 and COX-2 (Fig. 9-2). Each isoform is responsible for the production of certain prostaglandins. The COX-1 isoform catalyzes the production of prostaglandins that help regulate normal physiologic function, especially in the gastrointestinal (GI) and renal tracts. The COX-2 isoform facilitates the production of
inflammatory prostaglandins. Most NSAIDs block both the COX-1 and COX-2 isoforms of cyclooxygenase in a nonselective fashion.
inflammatory prostaglandins. Most NSAIDs block both the COX-1 and COX-2 isoforms of cyclooxygenase in a nonselective fashion.
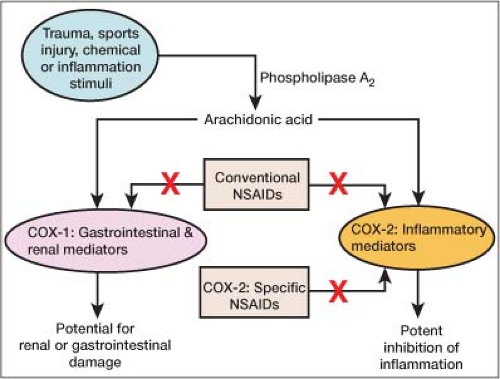 Figure 9-2 Cyclooxygenase cascade chart. Highlighting the difference between conventional NSAIDs & COX-2 specific NSAIDs. |
The goal for treating pain has been to block the COX-2 isoform responsible for the production of inflammatory prostaglandins without blocking the COX-1 isoform responsible for the production of the homeostatic prostaglandins. Although no NSAID is completely selective for the COX-2 isoform, NSAIDs more selective for the COX-2 isoform (COX-2 inhibitors) were developed to block inflammation and pain selectively without adversely affecting the homeostatic prostaglandins regulating the GI and renal tracts. Several NSAIDs significantly more selective for COX-2 inhibitors came to market, each with a different affinity for the COX-2 isoform. Nonselective NSAIDs like ibuprofen demonstrate a seven-fold increased affinity for the COX-2 isoform; Celebrex (celecoxib), a more selective COX-2 inhibitor, shows a 30-fold increased affinity, whereas Vioxx (rofecoxib, no longer on the market) was 200 times more selective for the COX-2 isoform.
After coming to market, some COX-2 inhibitors were shown to increase the rate of adverse cardiovascular events. One such drug was Vioxx, which was taken off the market in 2004. Celebrex, the only selective COX-2 inhibitor currently on the market, has been shown to be no different in increasing the rate of adverse cardiovascular events than Naprosyn (naproxen), an older, over-the-counter, nonselective NSAID.1 This could be explained by the fact that although Celebrex is more selective for the COX-2 isoform, it is not as potent as the previous COX-2 inhibitors. The severe imbalance in the prostaglandins produced because of Vioxx’s 200-fold greater affinity for the COX-2 isoform likely led to a state in which thromboxane, a proaggregatory and vasoconstrictive prostaglandin produced from the COX-1 isoform, went unchecked.2
Centrally, NSAIDs work by direct action on the CNS, altering spinal nociceptive processing. As peripheral impulses reach the spinal cord, their signals can be altered before they are sent to higher centers. This modulates the perception of pain. The exact mechanism of action of NSAIDs in the CNS is not known at this point.
When to Use
NSAIDs are indicated as first-line treatment for acute or chronic conditions exhibiting pain and inflammation. They can alleviate swelling, stiffness, joint pain caused by osteoarthritis, rheumatoid arthritis, and other rheumatic conditions. NSAIDs work well for muscle strain, inflammation of a tendon or ligament, bursitis, gout, dental problems, dysmenorrhea (menstrual pain), and metastatic bone pain.
NSAIDs start to work in about 30 minutes, with a peak effect in 60 to 90 minutes. They can be used as the sole agent or in combination with other pain medications. When combined with an opioid, they have been shown to reduce the amount of opioid need by 20% to 35%.3 The combination of an NSAID and opioid is known to have a synergistic effect—the whole is greater than the sum of its parts.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


