CHAPTER 46 NONOPERATIVE MANAGEMENT OF BLUNT AND PENETRATING ABDOMINAL INJURIES
BLUNT ABDOMINAL INJURY
Incidence
The incidence of intra-abdominal injury after blunt trauma will vary widely by the patient population, mechanism of injury, and the diagnostic studies employed by the particular center. Approximately 12% of all blunt trauma patients who are screened with computed tomography (CT) have one or more intra-abdominal injuries, with 46% of these being major injuries and 30% requiring surgical or angiographic intervention.1,2 The vast majority of these will be solid organ injuries to the spleen and/or liver, followed by injury to the kidney, mesentery, small bowel, colon, and pancreas. These injuries may be categorized as solid organ (liver, spleen, kidney), hollow viscus (stomach, duodenum, small bowel, colon, ureter, bladder), endocrine (pancreas, adrenal), or vascular. Overall, greater than 95% of these injuries may be managed without surgical intervention and with similar or lower complication rates compared with operative management.3
Mechanism of Injury
Blunt trauma may produce abdominal injuries through a variety of mechanisms, including direct transmission of energy to abdominal structures causing tissue disruption or hollow viscus blowout, shearing from rapid deceleration, direct compression of abdominal organs against the vertebral column, and puncture or laceration from associated rib fracture, spine fracture, or foreign bodies. Although there is not a linear relationship between the degree of force and the amount of abdominal injury, mechanisms involving higher velocity and/or forces will result in more significant and extensive injuries to the abdominal organs. Direct transmission of force to the abdomen will predominantly be absorbed by the large solid organs, such as liver, spleen, and kidney, resulting in parenchymal disruption. Rapid deceleration forces tend to affect fixed or tethered structures such as the kidneys, duodenum, and bowel mesentery, resulting in lacerations or pedicle avulsion. Although seat-belt use has resulted in a decrease in traumatic brain injury and death, there is a twofold increase in the incidence of hollow viscus injuries resulting from the use of seat-belts.3 Organs that are fixed to or in close proximity to the vertebral column may also be injured by direct compression, such as the distal duodenum, pancreas, and great vessels. Fractures of the lower rib cage may directly lacerate upper abdominal structures including the diaphragm, liver, spleen, and kidneys.
Diagnosis
The diagnosis of intra-abdominal injury in the blunt trauma patient begins with the primary survey and focused examination of the abdomen. Hypotension should be assumed to result from hemorrhage from an abdominal injury until proven otherwise. Physical examination of the abdomen may be limited by distracting injuries or depressed mental status, but should focus on the elicitation of peritoneal signs, localized tenderness, external bruising or evidence of a “seat-belt sign,” and distension.4 Peritonitis should never be attributed to a solid organ injury, as isolated hemoperitoneum should not cause diffuse peritoneal irritation. Focused abdominal sonography for trauma (FAST) is now commonly performed as part of the initial evaluation. While a “positive” FAST exam reliably identifies the presence of free fluid in the abdominal cavity suggestive of injury, a negative study does not exclude significant abdominal injury and should not be considered a definitive evaluation. Although ultrasound has been used to identify and grade specific organ injuries (i.e., liver and spleen), its reliability and reproducibility in this capacity has not been well demonstrated. Diagnostic peritoneal lavage (DPL) has largely been replaced by the FAST exam and CT scan and is rarely indicated, although it may be useful in select cases where there is suspicion for hollow viscus perforation with a compromised physical examination and equivocal CT scan findings. However, a diagnostic peritoneal aspirate (DPA) looking for the presence of gross blood only, can be very useful in the patient who is hypotensive with a negative FAST exam. A urinalysis should be obtained on all patients, and evaluation of the complete urinary tract (kidneys, ureters, bladder) should be performed in the presence of significant hematuria.
Computed tomography has become the standard of care for the definitive diagnosis of most blunt abdominal injuries, and should be used liberally. Missed intra-abdominal injuries, typically resulting from an incomplete diagnostic evaluation, represent the most common cause of preventable deaths from trauma.5 Modern generation helical CT scanners provide excellent detailed imaging of the abdominal organs, including retroperitoneal structures and major vasculature. It has a sensitivity and specificity approaching 100% for solid organ injuries, and provides anatomic detail that is invaluable for injury grading.1,3 The abdominal CT scan should always be performed using intravenous contrast if possible, as a “contrast blush” can provide evidence of active bleeding or arteriovenous fistula. Although some older series have characterized CT as unreliable for hollow viscus perforation or duodenal/pancreatic injury, more recent experience demonstrates that a high-quality CT scan will correctly identify most of these injuries. However, repeat CT imaging (if no other indication for laparotomy is present) or DPL should be considered in those infrequent situations with a high index of suspicion for missed injury or equivocal findings on the initial CT scan. We perform the abdominal CT scan with intravenous contrast only, as oral contrast has been shown to add little value in the trauma setting and may create undue delay as well as risk aspiration. Oral contrast may be useful when obtaining a delayed CT scan to evaluate for hollow viscus perforation, or to better delineate known or suspected pancreatic or duodenal injuries.
Anatomic Location of Injury and AAST-OIS Grading
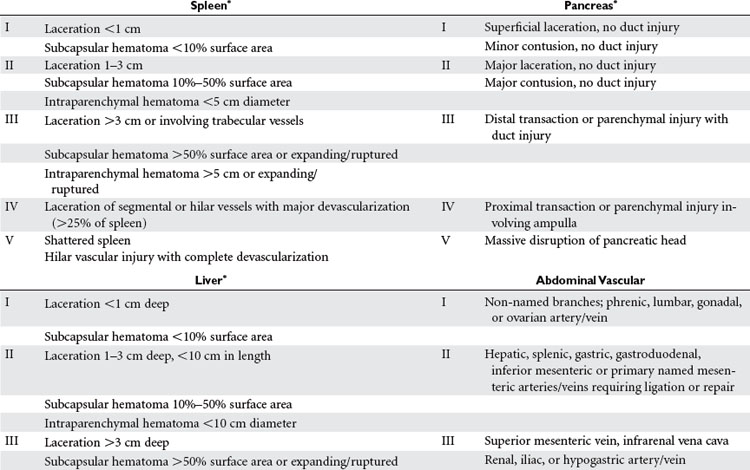
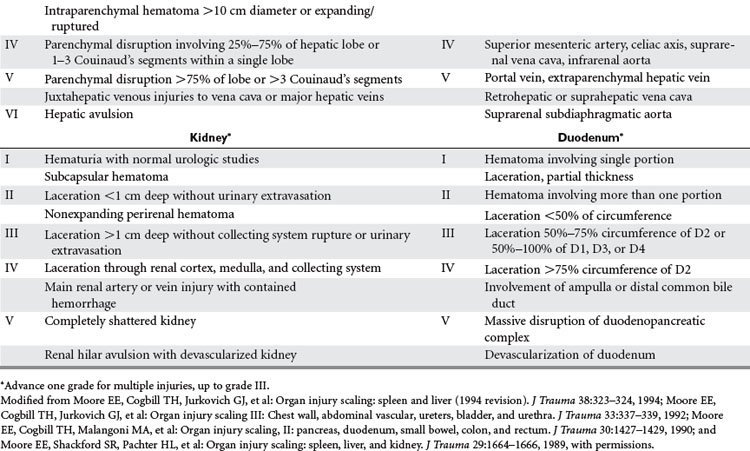
Abdominal injuries identified by CT should be graded according to the American Association for the Surgery of Trauma–Organ Injury Scale (AAST-OIS system) (Table 1). This provides a commonly understood language for discussion and study of these injuries, and may be used to guide the level and duration of monitoring for nonoperative management. Although higher-grade injuries are associated with higher rates of morbidity and failure of nonoperative management, the grade of injury should not be the primary factor in this decision. All grades of injury may be successfully managed nonoperatively in the appropriate clinical setting. Additional factors such as the amount of hemoperitoneum, presence of associated injuries, and presence of a contrast “blush” should be noted and factored into subsequent management decisions.
Management
Initial management decisions in patients with a known or suspected intra-abdominal injury should be based on the clinical examination and hemodynamic status. Patients with peritonitis or hemodynamic instability that persists despite adequate fluid resuscitation should undergo prompt exploratory celiotomy. Fluid resuscitation in the early evaluation period should be administered judiciously and only if necessary. Overzealous volume resuscitation with elevation of the mean arterial pressure may exacerbate hemorrhage from the injured organ or may cause an iatrogenic drop in the hemoglobin by hemodilution, which may be difficult to differentiate from active bleeding. We prefer small-volume boluses with immediate assessment of the patient’s response by an experienced trauma surgeon. There is a mounting body of evidence that supports the positive resuscitation and immunomodulatory benefits of hypertonic crystalloid solutions over standard crystalloid or colloid formulas.6 Administration of small boluses of hypertonic fluid (100 cc–250 cc of 3%–7.5% saline) will result in decreased tissue edema with improved gas exchange, a decreased systemic and organ-specific inflammatory response, with an excellent safety profile. In patients with associated traumatic head injury, hypertonic saline has the added benefit of lowering intracranial pressure while volume resuscitating the patient.
The primary components of safely managing these injuries are appropriate monitoring and frequent reassessments of the patient’s clinical exam and laboratory values. The level of inpatient care (intensive care unit [ICU] versus ward) and the frequency of monitoring should be dictated by the patient’s clinical status, associated injuries, and the severity of the organ injury. All personnel caring for the patient should be made aware of the presence and type of abdominal injury, and a clear plan for monitoring and alerting the trauma team to any changes should be in place. Most injuries that fail nonoperative management will declare themselves within 48 hours of injury, and this should be the period of most intensive monitoring.
Additional important factors to be considered in guiding management are the age of the patient and the presence of comorbidities and associated injuries. Traditionally, nonoperative management of abdominal solid organ injuries was contraindicated in elderly patients and those with multiple associated injuries, particularly severe traumatic brain injuries. However, with improvements in imaging technology and monitoring capabilities, many centers are reporting favorable results of nonoperative management in these more difficult patient populations.7,8 Success rates for nonoperative management of over 90% have been reported among patients with multiple associated injuries, with similar complication rates to those with isolated injuries.9,10 This should only be attempted at centers with experience and expertise in managing complex, multisystem trauma and requires coordination and cooperation between the involved surgical services, such as neurosurgery and orthopedics.
Spleen and Liver
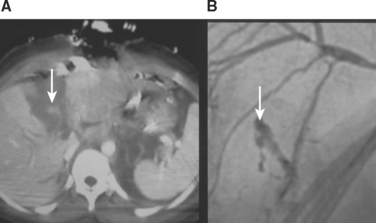
Patients with any identified injury of the spleen and/or liver should be admitted to the hospital for a minimum of 24–48 hours of observation. We recommend ICU or intermediate-level (step-down) admission for all high-grade injuries (grades III through V) (Figures 1 and 2). The primary purpose of observation is to identify the presence of any associated abdominal injuries and to monitor for ongoing or recurrent bleeding from the liver or spleen. The overall incidence of missed injuries in these patients appears to be low (around 2%), and should not influence the decision for nonoperative management.5,11 Serial physical examinations should focus on the patient’s hemodynamic status and any evidence of worsening abdominal tenderness, distension, or the development of peritonitis. Serial laboratory evaluations should include a complete blood count at the minimum. Some measure of global tissue perfusion and acidosis, such as the lactate or base deficit, may be useful in making management and treatment decisions in these patients. The timing and appropriateness of blood transfusion in these patients remains an area of controversy. Although the need for transfusion was previously used as a guideline for operative intervention, this is no longer the case. For spleen injuries, we favor a low threshold for operative or angiographic intervention if the patient requires more than one to two units of transfused blood. We accept a higher threshold for surgical intervention on liver injuries that require transfusion, typically after four to six units of transfused blood. Ideally it would be preferred if one could avoid transfusion and surgery, but the exact timing of transfusion, surgery, or both for patients with solid organ injuries remains more an art than science. It requires the expert judgment of an experienced trauma surgeon to avoid the error of delaying a needed laparotomy until the patient is on the verge of hemodynamic collapse.
Kidney
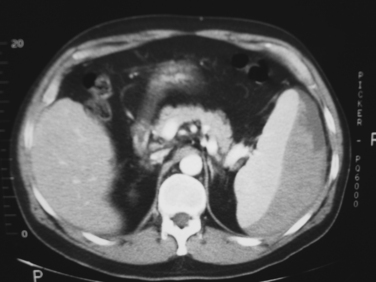
The kidneys are highly amenable to nonoperative management of most blunt injuries, with successful nonoperative management reported in over 90% of injuries and even in up to 50% of grade V injuries.12,13 This is particularly important for preserving renal function, as a significant number of surgical explorations for blunt renal injury will result in nephrectomy. Tamponade of hemorrhage from the renal parenchyma is enhanced by the tough, fibrous capsule of the kidneys (Gerota’s fascia) and their retroperitoneal location. The principles of hospital admission, monitoring, and serial evaluations are the same as for liver and spleen injuries. In addition to serial hemoglobin assessments for bleeding, measures of renal function (blood urea nitrogen, creatinine, creatinine clearance) should be obtained at admission and intermittently throughout the hospital stay. A urinary catheter should be placed to quantify urine output and the degree of hematuria (if present) in the initial observation period. We recommend liberal use of repeat imaging, including renal function studies, in patients with grades III through V injuries to assess the extent of injury and amount of functional renal parenchyma remaining (Figure 3).

Duodenum and Pancreas
Injury to the duodenum or pancreas is rare after blunt trauma, and appears to occur more frequently in children compared with adults. Diagnosis of these injuries is difficult because of their retroperitoneal location, often subtle clinical signs, and frequent poor visualization by CT scan. Unlike other abdominal organ injuries, most identified duodenal and pancreatic injuries will require operative exploration for repair and drainage. However, select lower-grade injuries may be amenable to successful nonoperative management. Most grade I injuries of the duodenum (hematoma or partial-thickness laceration) do not require laparotomy and will resolve spontaneously. Patients with a large intramural hematoma, particularly children, may experience obstructive symptoms and require hospitalization for nutritional management until the hematoma shrinks and obstruction resolves. Repeat imaging with oral contrast may be helpful in these patients to assess the degree of luminal obstruction and resolution or progression of the lesion.
Related posts:
 THE DEVELOPMENT OF TRAUMA SYSTEMS
THE DEVELOPMENT OF TRAUMA SYSTEMS
 DELIVERING MULTIDISCIPLINARY TRAUMA CARE: CURRENT CHALLENGES AND FUTURE DIRECTIONS
DELIVERING MULTIDISCIPLINARY TRAUMA CARE: CURRENT CHALLENGES AND FUTURE DIRECTIONS
 GASTRIC INJURIES
GASTRIC INJURIES
 PALLIATIVE CARE IN THE TRAUMA INTENSIVE CARE UNIT
PALLIATIVE CARE IN THE TRAUMA INTENSIVE CARE UNIT
 TRAUMATIC BRAIN INJURY: PATHOPHYSIOLOGY, CLINICAL DIAGNOSIS, AND PREHOSPITAL AND EMERGENCY CENTER CARE
TRAUMATIC BRAIN INJURY: PATHOPHYSIOLOGY, CLINICAL DIAGNOSIS, AND PREHOSPITAL AND EMERGENCY CENTER CARE
 NOSOCOMIAL PNEUMONIA
NOSOCOMIAL PNEUMONIA
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


