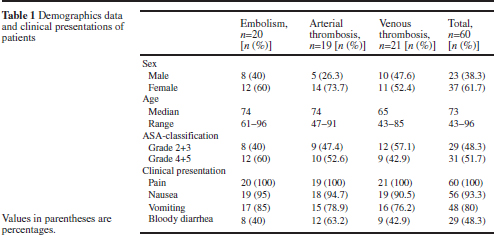
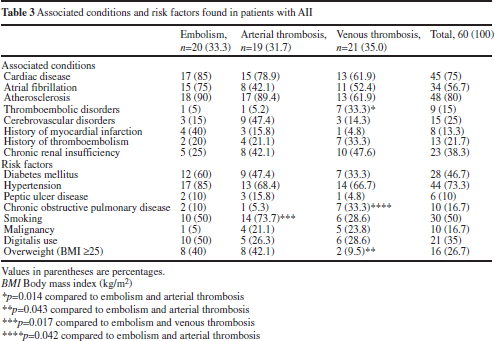
Chapter 27 Mesenteric ischemia often presents as a sudden and catastrophic illness with a very high mortality rate despite medical and surgical therapy. Understanding the anatomy and pathophysiology provides the background for guiding diagnosis and management. The prevalence of mesenteric vascular disease as well as the clinical, laboratory, and radiologic features supporting prompt diagnosis will be presented. Evolving medical as well as open and endovascular surgical treatment will be reviewed. The embryonic intestines grow more quickly than the body of the fetus. As a result they protrude through the umbilical ring. They are supplied primarily by the Vitelline artery, which will become the superior mesenteric artery (SMA). After the 6th week the intestines rotate counterclockwise 90° and the cranial limb, the future small intestine now lies to the right side. It elongates and forms a number of loops. The shorter left side caudal limb will become the large intestine. After 10 weeks the intestines return to the abdominal cavity and undergo a further counterclockwise rotation of 180°. The small intestine returns first followed by the large intestine which now forms its characteristic loop, lying anterior to the SMA. The small intestine and right colon are supplied by the SMA. The celiac trunk supplies the duodenum as well as some potential collateral supply at the ligament of Treitz through the pancreatico-duodenal artery (via the right hepatic artery). The inferior mesenteric artery supplies the left colon. There is variable collateral supply to the transverse colon through the marginal artery of Drummond. The terminal branch of the inferior mesenteric artery supplies the proximal rectum. Distally the rectum is supplied by the inferior and middle rectal arteries, which originate from the Internal Iliac. Collateral supply between the superior and inferior rectal arteries is usually good. Both the superior and inferior mesenteric arteries fan out into arcades. Their terminal branches are the vasa recta. The mesenteric branches are short, the anti-mesenteric branches are long and as a result the anti-mesenteric side has a more tenuous blood supply. The venous drainage parallels the arterial anatomy. The inferior mesenteric artery drains into the distal splenic artery. The superior mesenteric vein passes posterior to the head of the pancreas where it joins the splenic vein to form the portal vein. The only jejunal, ileal, and colonic direct venous drainage to the vena cava is via collaterals distally through the middle and inferior rectal veins. The anatomy of the arterial and venous systems dictates the distribution of ischemia with arterial or venous disorders. The abrupt angled origin of the celiac artery protects it from most embolic events. Emboli are more likely to pass through the SMA, which, has a large orifice and has a wide proximal angle of takeoff from its origin at the aorta. A smaller orifice protects the inferior mesenteric artery and the left colon benefits from collateral supply via the inferior and middle rectal arteries. The venous drainage via the portal system results in thrombosis associated with diseases that affect hepatic drainage or predispose to hepatic and splenic vein thrombosis. The development of atherosclerotic disease may promote development of collateral supply to the proximal small bowel and transverse colon via the celiac artery and its branches. More often however, collateral supply from the inferior rectal arteries as well as through the marginal artery of Drummond is compromised. The watershed area at the Arc of Riolan (splenic flexure) is particularly at risk.1 Mesenteric ischemia is frequently encountered by busy emergency general, colorectal and vascular surgical services as well as critical care practitioners. Atherosclerosis increases with age and is prevalent in over 20% of patients aged 65 and greater. The majority of patients with atherosclerosis involving the mesenteric arteries are asymptomatic. A population study in Malmo, Sweden is illustrative. Over a 12-year period the hospital autopsy rate was over 80%. The incidence of mesenteric ischemia at surgery or autopsy was 12.9/100,000 person years. Two thirds had an acute SMA occlusion, nearly 1/3 were divided equally between mesenteric vein thrombosis and nonocclusive ischemia. The disease was distributed equally between men and women.2 In cases of SMA occlusion, thrombosis was four times as common as embolic occlusion. The thrombi were both more proximal and more extensive resulting in greater intestinal necrosis. Arterial emboli were frequently multiple and could be suggested by the presence of other solid organ infarcts on CT, at surgery or on autopsy. Non-occlusive ischemia was associated with congestive heart failure, dysrhythmias and a history of recent surgery. These patients had a terrible prognosis reflecting their co-existent disease. Mesenteric thrombosis was associated with thrombophilia and thromboembolic disease. Another large series from Leipzig, Germany summarized the characteristics of thrombotic intestinal ischemia (embolic and thrombotic) over a 6-year period. Arterial emboli, arterial thrombosis and venous thrombosis each were responsible for a third of the patient presentations. The overall mortality was 60%.3 Fig. 1. Demographic and clinical features. Source: Table 1, Demographics, mesenteric ischemia.3 Table 2 Laboratory test results at initial presentation Values represent mean ± SEM. Fig. 2. Laboratory findings. Source: Table 2, Demographics, mesenteric ischemia.3 Fig. 3. Associated conditions and risk factors. Source: Table 3, Demographics, mesenteric ischemia.3 Mesenteric Ischemia includes four distinct presentations: Arterial emboli Arterial thrombosis Venous thrombosis Non-occlusive mesenteric ischemia (acute and chronic)
Mesenteric Ischemia
John B. Kortbeek
Introduction
Anatomy
Epidemiology
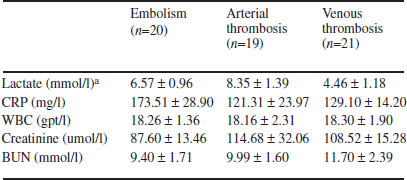
CRP C-reactive protein, WBC white blood cell count, BUN blood urea nitrogen
aValues of lactate were available for 46 patients.
Classification and Pathophysiology
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


