93 Mechanical Support in Cardiogenic Shock
An estimated 61.8 million people in the United States have heart disease, among whom 950,000 die annually.1 Of these, 540,000 people suffer myocardial infarctions each year; 193,000 succumb to complications directly related to the infarction. The leading cause of death among hospitalized patients with acute myocardial infarction (AMI) continues to be cardiogenic shock.2 The incidence of cardiogenic shock complicating AMI (approximately 7%) has remained constant over the past 25 years. Accurate statistics on the worldwide utilization of all mechanical support for cardiogenic shock are not known. However, estimates on the use of intraaortic counterpulsation for patients in shock after AMI suggest a rate of use in only 22% of eligible patients.3 The reasons for the apparent underutilization of this readily available modality are not clear. Accordingly, the indications, benefits, and limitations of mechanical cardiac support are outlined in this chapter.
 Historical Background
Historical Background
The evolution of mechanical cardiac support dates to the early 1950s when Gibbon developed the prototype cardiopulmonary bypass (CPB) apparatus.4 In the years following, Lillehei, Kirklin, and others applied the heart-lung machine to facilitate open-heart surgery; their pioneering work and early observations led directly to the development of modern mechanical cardiac support systems.5–7 These surgeons recognized that some patients had improved outcomes after surgery if they were weaned slowly rather than abruptly from CPB support. Their initial publications introduced the concept that left ventricular (LV) decompression and myocardial rest could afford enhanced cardiac recovery after the insult of open-heart surgery. Clinical use of extracorporeal CPB for heart surgery became widespread in the early 1960s. Simultaneously, several groups of investigators were testing means of mechanical cardiac assistance for use outside the operating room for support of patients in cardiogenic shock. The current modes of mechanical support are derivations of those originally developed and include aortic counterpulsation, continuous flow pumps with or without an oxygenator, and pulsatile pumps.
History of Aortic Counterpulsation
The concept of arterial counterpulsation was introduced in 1961 by Clauss and coworkers and involved use of an external “ventricular” chamber that filled with blood from a catheter in the iliac artery8 and was subsequently compressed by a piston. Compression of the “ventricle” was synchronized to either the QRS complex of an electrocardiogram (ECG) or the impulse of a pacemaker, so that a counter pulse of blood was delivered into the arterial system during diastole. It was demonstrated in dogs that cardiac stroke work and LV end-systolic pressures could be substantially reduced with the use of a counterpulsation into the aorta. The following year, Moulopaulus and associates adapted the model to create an intraaortic balloon pump (IABP) that could provide a similar counterpulsation without the need for blood reservoirs.9 The investigators used a balloon that was rapidly inflated and deflated with carbon dioxide during native diastole. The IABP was subsequently adapted and described for clinical use by Kantrowitz and colleagues in 1968.10
The physiologic rationale for the efficacy of the IABP is that balloon deflation provides a rapid, synchronized reduction in impedance (afterload) during isovolemic LV contraction. This is followed by a rapid, synchronized increase in aortic pressure during isovolemic LV relaxation (diastolic augmentation) caused by balloon inflation. In combination, these events achieve two important goals. First, LV systolic unloading directly reduces stroke work, which in turn reduces myocardial oxygen consumption during the cardiac cycle. Second, diastolic augmentation raises arterial blood pressure and provides better coronary arterial perfusion during diastole, yielding increased oxygen delivery to the myocardium. The IABP does not directly move or redistribute blood flow; however, peak diastolic coronary flow velocity can be increased as much as 87% with IABP augmentation and peak diastolic flow velocity by as much as 117%.11 Since introduction into clinical use in 1968, the IABP has remained an important adjunct to supporting patients in cardiogenic shock. Myocardial recovery is promoted by the reduction of cardiac work and the simultaneous increase in myocardial oxygen supply. However, therapeutic success is dependent on the patient having a minimum degree of LV function that, in combination with IABP support, facilitates an adequate cardiac output to sustain end-organ function. When this minimal cardiac output is not met, alternative mechanical cardiac assistance must be considered.
History of Mechanical Assist Devices
The need for effective mechanical cardiac assist devices became apparent in the 1950s during the development of CPB for open-heart surgery. Initial attempts with prolonged postoperative CPB demonstrated that the bypass circuit was damaging to both end-organ function and blood constituents after several hours of use.12 The first attempt at isolated extracorporeal LV support was with a simple roller pump in 1962.13 Subsequently, femoral venous–to–femoral arterial CPB was successfully used by Spencer and colleagues in four patients with postcardiotomy cardiac failure.14
Simultaneous to Spencer and colleagues’ work with extracorporeal systems, DeBakey designed the first intracorporeal LV assist device (LVAD), the DeBakey blood pump.15 This device consisted of a Dacron-reinforced silicone rubber tube with an inner chamber of blood from the left atrium that was connected to the descending thoracic aorta. Pressurized air was instilled into the outer chamber by an external pneumatic controller to compress the inner blood chamber, timed to the R wave of the QRS complex. Blood flow was directed from the left atrium to the descending aorta with the use of ball valves at both the inflow and outflow ends of the device. The DeBakey blood pump was first used in a patient who died 4 days postoperatively of neurologic complications. A remodeled extracorporeal version was subsequently used for postcardiotomy failure in a 37-year-old woman after aortic and mitral valve replacements. The device was needed for 10 days, but the patient survived.16
By 1972, investigators at the Texas Heart Institute had developed a pneumatically driven LVAD designed to be implanted in the abdomen.17 This device had a blood chamber compressed by pulses of air delivered into the pump by a percutaneous driveline. Modern devices have chamber compression that is electrically powered via percutaneous drivelines. Paracorporeal, pneumatically driven devices were a parallel development. Paramount to the evolution of these devices was the sponsorship of the Artificial Heart Program of the National Heart, Lung, and Blood Institute, which was chartered in 1964.
By the 1960s, continuous flow, as compared to pulsatile, pumps were under development.18,19 Over the subsequent 15 years, centrifugal pumps were perfected and introduced into clinical use. These pumps work on the principle of a forced, constrained vortex devised from three magnetic cones.20–22 They have been shown to be useful in a variety of clinical settings where short-term mechanical support is needed and an IABP is inadequate. Several types of small, axial-flow or rotary pumps have also been developed, including some that allow for percutaneous deployment.23–36 These are generally constructed of a magnetically suspended impeller that rotates at extremely fast rates (25,000 to 35,000 rpm). The axial rotary pump technology has some potential advantages over pulsatile devices; they are quite small with few moving parts and do not require a compliance chamber. The latest generation of rotary pump technology utilizes fully magnetically levitated rotors that completely eliminate the need for seals or bearings. This technology reduces the risk of damage to blood elements and may lead to lower rates of thromboembolism.
 Current Mechanical Support Devices
Current Mechanical Support Devices
Counterpulsation/Intraaortic Balloon Pump
Indications
The absolute indications for IABP placement include cardiogenic shock, uncontrolled angina pectoris, acute postinfarction ventricular septal defect or mitral regurgitation, and postcardiotomy left-sided heart failure with low cardiac output. In these settings, IABP should be considered a primary therapy that should not be delayed until noncardiac injury is clinically evident. It is important to recognize that blood pressure alone is not an adequate indication of hemodynamic or cardiac stability. Limb perfusion, renal function, mental status, and even gastrointestinal function need to be considered in the assessment of adequate resuscitation and homeostasis. Additional measurable indices include arterial (SaO2) and mixed venous oxygen saturation (SvO2), acid-base status, urine output, and body temperature. A multivariate analysis of data accrued from 391 postcardiotomy patients requiring IABP demonstrated that epinephrine requirements greater than 0.5 µg/kg/min, a left atrial pressure greater than 15 mm Hg, urine output less than 100 mL/h, and SvO2 less than 60% correlated with mortality.37 These criteria were used to help predict mortality and the need for subsequent mechanical support.
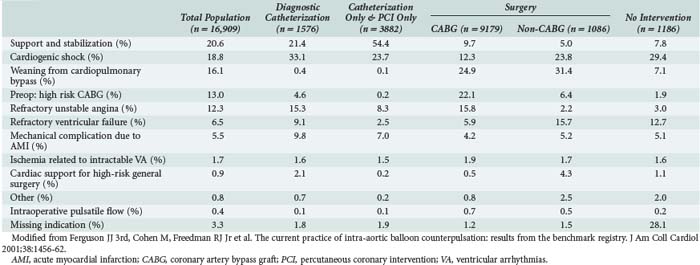
Other relative indications for IABP use include (1) high-risk, catheter-based interventional procedures such as left main coronary artery angioplasty, (2) after unsuccessful attempts at catheter-based intervention in patients with poorly controlled ventricular arrhythmias, and (3) concomitant poor LV function, and (4) in settings of persistent stunned, ischemic myocardium. These are all circumstances in which reduction of LV systolic wall tension and oxygen consumption by the IABP might enhance myocardial recovery after intervention. Conversely, the use of an IABP had no impact on mortality in a population of patients without hemodynamic instability undergoing high-risk angioplasty randomized in a prospective trial reported in 1997.38 More recently, the Benchmark Counterpulsation Outcomes Registry of IABP use in 22,663 patients from 250 hospitals worldwide demonstrated that cardiogenic shock and high-risk angioplasty were the most common indications for utilization of the device.39 Table 93-1 depicts a further characterization of the Benchmark report with respect to indications for use of the IABP and subsequent interventions.40 Nevertheless, despite the widespread use of the IABP in over 150,000 patients worldwide each year,41 no prospective randomized trial has ever demonstrated a survival benefit with IABP use in the patient population undergoing high-risk catheter intervention. In contrast, the SHOCK trial showed that early revascularization of patients with coronary artery disease and shock after an AMI, often facilitated by IABP use (86%), yielded a lower 6-month mortality rate (50%) than with medical therapy alone (63%).2 Additional studies have shown that in patients undergoing urgent or emergent revascularization after an AMI, those supported preoperatively with an IABP had a lower operative mortality than those in whom an IABP was not used (5.3%-8.8% versus 11.8%-28.2%).42,43 These data seem to justify a strategy of aggressive IABP use to facilitate early revascularization in the postinfarction patient.
Technical Considerations
The optimal site of insertion of an IABP is a common femoral artery that can be accessed either percutaneously with the use of a guidewire or by surgical cutdown. Modern intraaortic balloon catheters are available for adults and children according to the appropriate size and length for a given height and weight of the patient. Adult intraaortic balloons have a range in volume filled between 25 and 50 mL, with a standard balloon size holding 40 mL of helium. IABP catheters placed through the femoral artery are positioned so that the tip is just distal to the takeoff of the left subclavian artery in the proximal descending thoracic aorta. Optimally, the tip of the catheter should be positioned with transesophageal echocardiographic (TEE) or fluoroscopic guidance.44 To reduce the diameter of femoral cannulation, a sheathless IABP technique can be utilized and is our preferred method.45
Inflation of the balloon should be timed with closure of the aortic valve (at the dicrotic notch of the aortic pressure tracing) and should be inflated to nearly occlude the descending thoracic aorta. Timing can be synchronized in one of three ways: (1) using an arterial (preferably aortic) pressure tracing in synchrony with the dicrotic notch, (2) using the descent of the R wave on a rhythm tracing, or (3) timed after a ventricular pacing spike when a pacemaker is in use.46–50 The effectiveness of IABP is significantly improved by proper timing of inflation and deflation, which can be difficult when there is an accelerated heart rate, cardiac rhythm disturbances, atrioventricular dyssynchrony, or low mean arterial pressure. IABP timing should be adjusted to maximize diastolic augmentation; hence, deflation should be as late as possible but just before opening of the aortic valve. If this cannot be gauged by the pressure tracing, it can be timed to the onset of the R wave on the ECG tracing or with the use of M-mode echocardiography.51
When femoral arterial cannulation is not desirable because of aortoiliac occlusive disease or extensive peripheral vascular disease, the subclavian artery or the ascending aorta can be utilized.52–56 With either technique, the IABP catheters are advanced antegrade down the descending thoracic aorta so that the balloon tip sits above the level of the diaphragmatic hiatus, and the most proximal end of the balloon is distal to the takeoff of the left subclavian. These antegrade balloons should always be placed with either fluoroscopic or echocardiographic guidance. They should be removed with open arterial repair in all cases.
Complications
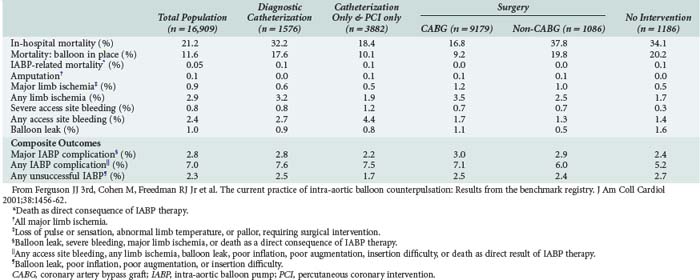
The overall complication rate of IABP utilization is between 5% and 10%. Major complications occur at a rate of about 3% and include severe bleeding, major limb ischemia or amputation, infection, visceral or spinal cord ischemia, and attributable IABP mortality.39,43 A summary of IABP complications as they occur in relation to subsequent percutaneous or operative coronary revascularization from the Benchmark Registry are listed in Table 93-2.40 In this registry, rates of complications were quite low, the most common being access-site bleeding (4.3%) and limb ischemia (2.3%).39 The rates of amputation, stroke, visceral or spinal cord ischemia and IABP-related mortality are all 0.1% or less.39 Intraaortic balloon entrapment is a rare complication.57–59 The incidence of major vascular complications according to the STS National Database (1996-1997) and the Benchmark Registry (1997-1999) is 5.4% and 1.4%, respectively.40,43 Ipsilateral limb ischemia should be immediately addressed after its recognition. This usually requires removal of the IABP, with replacement at another location if it is still indicated. The ischemic limb may require thrombectomy with or without revascularization and fasciotomy.60–66
Outcomes
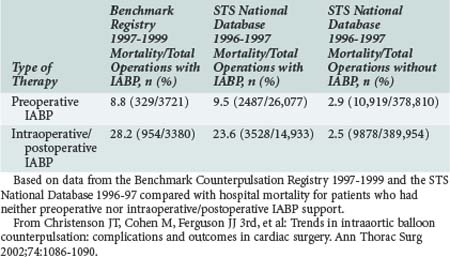
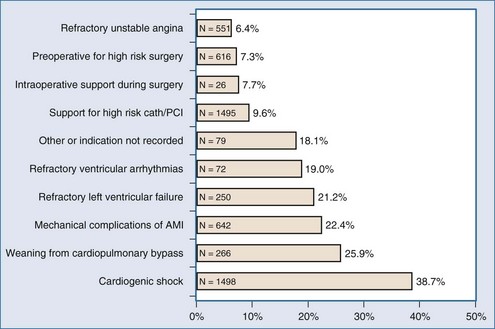
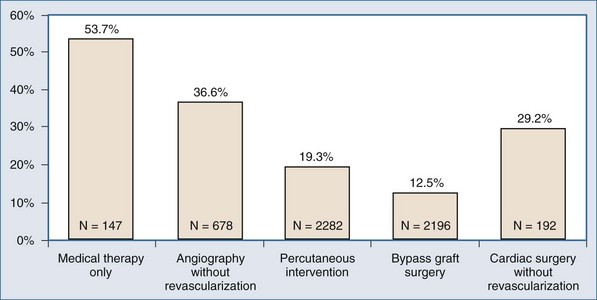
In the absence of prospective randomized data, it is difficult to ascribe outcome secondary to IABP placement. The Second Angioplasty in Myocardial Infarction (PAMI-II) Trial data examined high-risk patients with acute myocardial infarction revascularized by percutaneous intervention only and demonstrated a modest survival advantage at 6 months with the use of periprocedural IABP support.38 When evaluating hospital mortality rates among patients undergoing coronary artery bypass graft (CABG) and/or valve surgery who received preoperative IABP or required intraoperative/postoperative IABP support, it is evident that mortality was significantly lower among patients supported preoperatively, as depicted in Table 93-3.40,43 Hence, there appears to be a survival advantage to earlier IABP support for patients with AMI and cardiogenic shock who need revascularization. In the setting of an acute ventricular septal defect (VSD) or acute mitral regurgitation after an AMI, IABP support can offer a dramatic improvement in the hemodynamic response of the patient.67–71 Figures 93-1 and 93-2 stratify hospital mortality rates associated with IABP use in patients with AMI by principal usage indication or by performance of percutaneous or surgical coronary revascularization. It is clear that the mortality rate of cardiogenic shock after AMI remains high at 39%. However, IABP support combined with revascularization portends a better prognosis than adjunctive IABP use with medical therapy alone.39
TABLE 93-3 Hospital Mortality (Outcome Parameter) for Patients Undergoing Cardiac Surgery Who Either Received Preoperative IABP or Intra-/Postoperative IABP Support
Continuous Flow Pumps
Both roller pumps and centrifugal pumps deliver continuous flow but have other distinct limitations. Roller pumps remain in widespread use for cardiopulmonary support during cardiac surgery; applications outside the operating room have been virtually abandoned for several reasons. Roller pumps are insensitive to changes in arterial line resistance that may cause disruption of the apparatus. They require unobstructed venous flow. The rollers eventually cause spallation of tubing, leading to particle emboli and weakening of the tubing.72 Roller compression causes hemolysis after prolonged use.73 Alternatively, centrifugal pumps are sensitive to both outflow resistance and filling pressure, offering a safer applicability outside the operating room. Centrifugal pumps like the BioMedicus Bio-Pump (Medtronic Corp., Minneapolis, Minnesota) generate a constrained vortex within an acrylic shell that houses concentric magnetic cones. The cones rotate as a magnetic rotary motor spins adjacent to the base of the cones20–22 and can generate very high flows with less trauma to blood cells than roller pumps.73–75
The technology of centrifugal pumps, axial flow pumps, and membrane oxygenators has remarkably improved. Pump durability and reduced blood cell trauma have been demonstrated.19,26,73–76 As a result, considerable experience has accumulated with the use of centrifugal pumps (cardiopulmonary support) for postcardiotomy LV failure, fulminant myocarditis, or cardiogenic shock after AMI.32,77–93 Newer devices have incorporated design modifications that allow for improved pump performance as well as percutaneous application.
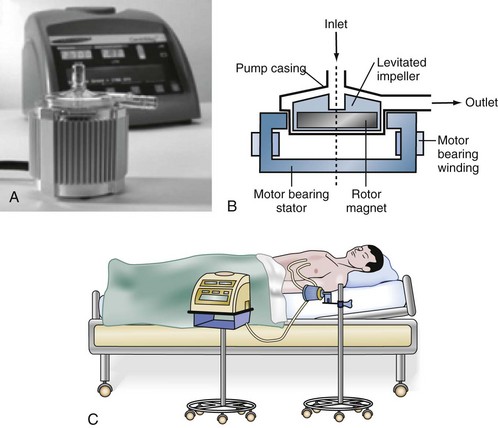
A novel centrifugal blood pump, the CentriMag system, utilizes fully magnetically levitated technology (Figure 93-3) to provide external mechanical circulatory support in a fashion similar to the BioMedicus Bio-Pump. The CentriMag system has many advantages that make it attractive for short-term mechanical support in the acute setting.94 These advantages include ease of implantation, direct outflow cannulation of the ventricle for improved decompression, minimal need for anticoagulation, and less damage to blood elements compared to traditional devices such as the BioMedicus pump. It has been used effectively for uni- or biventricular support in the setting of postcardiotomy cardiac failure as a bridge to decision, recovery, or long-term mechanical circulatory support device. For patients who also require pulmonary support, an oxygenator may be added to the circuit, effectively converting it to an ECMO system.
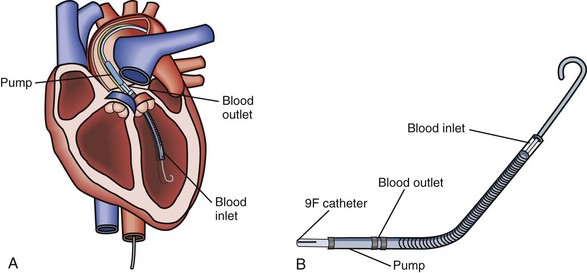
The Tandem Heart System (Cardiac Assist Inc., Pittsburgh, Pennsylvania) is an external centrifugal pump system that allows for percutaneous LV support (Figure 93-4).95 Utilizing a percutaneous venous cannula that crosses the atrial septum, this pump can provide LV assistance without performing a sternotomy. This device has been utilized both for short-term support in the catheterization suite or as a bridge to recovery, more definitive mechanical circulatory support (i.e., implantable device), or transplantation.
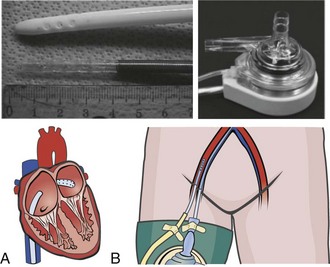
The most recent addition to the armamentarium for acute short-term mechanical circulatory support is the Impella Recover axial flow pump (Abiomed Inc., Danvers, Massachusetts). This device can be placed percutaneously or directly via the open chest during cardiac surgery (Figure 93-5). It has been used for partial support during percutaneous coronary interventions as well as for postcardiotomy cardiogenic shock as a bridge to recovery or a more definitive long-term device.96 Important limitations for the use of this device include aortic stenosis that precludes proper positioning of the device as well as peripheral vascular disease that may make percutaneous deployment impossible or mandate a surgical cutdown for placement. This device cannot be used in patients who have had a previous mechanical aortic valve replacement.
Indications
Short-term cardiopulmonary support for cardiogenic shock has emerged as an important adjunctive therapy. It is a relatively simple means of establishing immediate and complete circulatory support, requiring no additional equipment other than that needed for standard CPB support during cardiac surgery. Cardiopulmonary support can be initiated percutaneously via the common femoral artery and vein. Alternatively, when faced with postcardiotomy LV failure, cardiopulmonary support can facilitate patient stabilization for subsequent transport to a tertiary medical center for VAD placement. Cardiopulmonary support circuits can be converted to longer-term support (beyond 6-8 hours) by upgrading the oxygenator.97,98 A standard microporous hollow-fiber oxygenator (the type used in most CPB circuits) has a lifespan of 6 to 12 hours.99 Changing to a solid-silicone membrane oxygenator (not microporous) will lengthen the lifespan of the cardiopulmonary support circuit up to 21 days; this conversion constitutes extracorporeal membrane oxygenation (ECMO) support. ECMO is generally used in the adult population for periods of 1 to 10 days when there is marked concomitant pulmonary insufficiency and cardiac failure. ECMO is also used for short-term (1-3 days) support when the neurologic status of a patient is unclear and longer-term support (i.e., VAD support) may not be appropriate until this status is clarified. Thus, ECMO can be used as a bridge to a longer-term, pulsatile flow assist device once the suitability of the patient is determined.
Technical Considerations and Complications
Disadvantages to the use of peripheral cardiopulmonary support or ECMO include the greater potential for ipsilateral limb complications, higher rates of hemolysis, the requirement for anticoagulation to prevent thrombosis of the oxygenator and circuit, and failure to adequately decompress the left ventricle.100–106 Inadequate LV decompression with peripheral cardiopulmonary support/ECMO systems may be the mechanism responsible for some treatment failures. Regardless of the etiology of cardiogenic shock, a rested ventricle (i.e., decompressed) has a better chance of recovery than a distended ventricle.
Outcomes
The use of ECMO in the adult population for reasons other than primary cardiac failure with secondary pulmonary insufficiency has limited advantages over conventional therapies.107,108 However, a substantial subset of patients who present with cardiogenic shock and are initially resuscitated with cardiopulmonary support/ECMO survive to revascularization, transplantation, or recovery, with survival rates as high as 75%.77,78,81,82,109–116 ECMO used as a bridge to VAD placement for profound cardiogenic shock (“double bridge” mechanical assistance) can yield survival rates greater than 40%.80 This strategy is pragmatic and offers immediate end-organ support while a subsequent definitive treatment plan can be designed.
Ventricular Assist Devices
Pulsatile Pumps
There is a growing body of evidence suggesting that pulsatile assisted circulation, in the setting of acute cardiogenic shock, offers improved end-organ perfusion and lymphatic flow and is thus beneficial.117–119 VADs that utilize direct cardiac outflow cannulation (VAD inflow) provide better ventricular decompression and rest than peripheral bypass support systems. There are now several mechanical assist devices that achieve these goals, including the extracorporeal ABIOMED AB 5000 (Abiomed) and the paracorporeal Thoratec VAD system (Thoratec Corp., Pleasanton, California). Two other implantable intracorporeal pulsatile VADs that were designed for patients with chronic heart failure may have roles in certain subsets of patients with acute cardiogenic shock. These are the HeartMate LVAS XVE (Thoratec) and the intracorporeal Thoratec VAD system (Thoratec).
Extracorporeal Short-Term Support
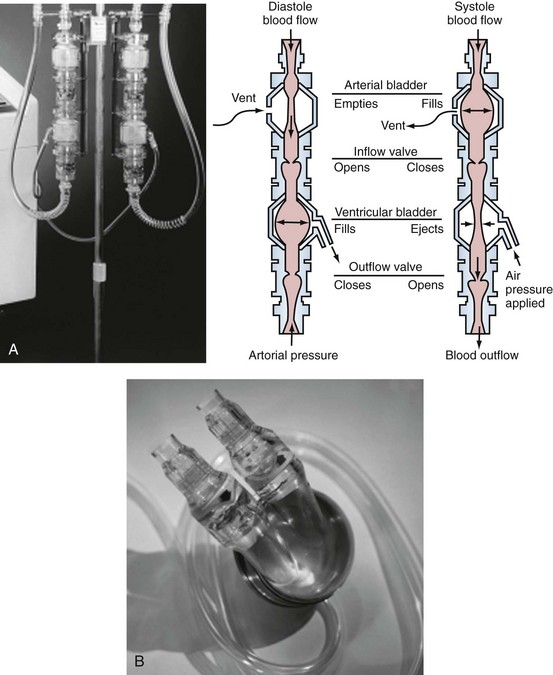
The recently FDA-approved ABIOMED AB 5000 “ventricle” replaces the previously utilized BVS 5000 which was developed in the 1980s and was granted approval for use for postcardiotomy heart failure by the U.S. Food and Drug Administration in 1992.116 Since that time, indications for the device have been broadened to include most patients with either postcardiotomy shock or precardiotomy shock who do not adequately respond to inotropes and an IABP. The ABIOMED system is a pneumatically driven, dual-chamber blood pump that delivers pulsatile flow. ABIOMED inflow cannulas are placed in the left and/or right atrium for univentricular or biventricular support. Outflow cannulas are housed with a Hemashield graft (Meadox Medicals Inc., Oakland California) and are sewn to the aorta and/or pulmonary artery for left-sided and/or right-sided heart support. The pumps, as depicted in Figure 93-6, are extracorporeal (BVS5000) or paracorporeal (AB5000). In the BVS5000, the upper (first) chamber fills passively by gravity, and the lower chamber serves as the pumping chamber. The two chambers are separated by a polyurethane trileaflet inflow valve; the lower chamber is separated from the arterial circulation by an outflow valve that prevents retrograde flow. As the pumping chamber is filled with blood, the surrounding air within the polycarbonate housing is displaced back into the drive console. This is sensed by the console; the console delivers compressed air back into the pumping chamber, which compresses the bladder and forces a pulse of blood into the arterial circulation.120 The stroke volume that results is 70 to 80 mL, with VAD output dependent on the rate of upper-chamber filling. The AB5000 “ventricle” has a single ventricular blood chamber that fills by vacuum assistance from a portable console. Blood is ejected by pneumatic inflation of polyurethane bladder housed within the pump casing. Valves constructed of Angioflex, ABIOMED’s proprietary polyether-based polyurethane plastic, insure unidirectional flow. Typically, flows of 5 L/min are achieved with either of the ABIOMED systems. Both of these devices require anticoagulation, particularly for LV assistance. The BVS5000 is generally useful for short-term (<7-10 days) support because of the increased risk of thromboembolic complications or device malfunction beyond this period. If longer support (2-3 months) is necessary, the ABIOMED pump can be exchanged with AB5000 or converted to a longer-term VAD system such as the Thoratec p-VAD or HeartMate.
< div class='tao-gold-member'>


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


