Fig. 26.1
Arrows demonstrate Right lower lobe consolidation (wide arrow) and Left Lower Lobe bronchiectasis (thin arrow)
The patient was transferred to intensive care. Flexible bronchoscopy showed no active bleeding but blood was seen in the superior segment of the RLL. Another episode of hemoptysis estimated at 500 ml occurred. The patient was positioned with his right side down and aggressively suctioned through the endotracheal tube. Selective intubation of the left mainstem bronchus was unsuccessful because of poor visibility due to blood in the airway and endotracheal tube.
Multi-detector computed tomography with contrast demonstrated right lower lobe consolidation and associated atelectasis. There was narrowing of the right upper lobe bronchus by soft tissue density (Fig. 26.2).
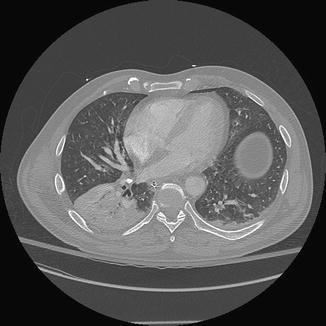
Fig. 26.2
Computed tomography image demonstrates dense right lower lobe infiltrate with broncholithiasis
Bronchial angiography was undertaken. The right and left bronchial arteries both arose from a single trunk. The left bronchial artery was relatively small with no abnormal vessels. On the right, the vessel divided into a branch to the upper lobe and a major lower lobe branch which was moderately enlarged with hyperemia in the lower lobe, associated with the area of consolidated lung. The right lower lobe bronchial artery was embolized and post embolization no flow in the right lower lobe bronchial artery was observed (Fig. 26.3).
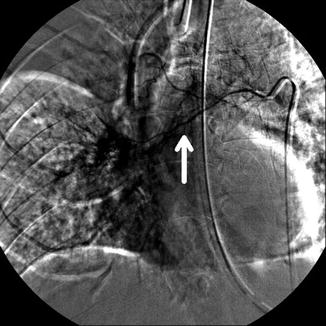
Fig. 26.3
Right Bronchial artery arteriogram demonstrates both upper lobe and lower lobe branch (arrow)
Soon thereafter, there was another episode of massive hemoptysis, which filled the ventilator circuit. This was associated with vasopressor-dependent hypotension, worsening hypoxemia and bradycardia.
A dual lumen endotracheal tube was placed, and both right and left sides were ventilated. The patient became more stable with decreasing vasopressor need. A right lower lobectomy was performed.
Principles of Management
Epidemiology
Massive hemoptysis occurs in about 5–15 % of all admissions for hemoptysis [1, 2]. Mortality was 7 % in a single center retrospective review of 1,087 patients [2] but has been reported as high as 75 % when the volume of hemoptysis exceeds 600 ml in 24 h. The wide range of mortality likely reflects the lack of a standard definition of massive hemoptysis as well as the variability in underlying etiology [3–5].
A scoring system to identify risk for mortality was derived from a 14 year experience of 1,087 patients admitted for hemoptysis, 717 of whom were admitted to the Intensive Care Unit (ICU), and 10 % of whom demonstrated massive hemoptysis with a mean cumulative volume of >200 ml. Risk factors include chronic alcoholism, ≥2 chest x-ray quadrants involved, pulmonary artery involvement, cancer, aspergillus infection or mycetoma, and initial mechanical ventilation. Two or more risk factors demonstrated a higher mortality [2]. (These risk factors are noted in the clinical algorithm, Fig. 26.4).
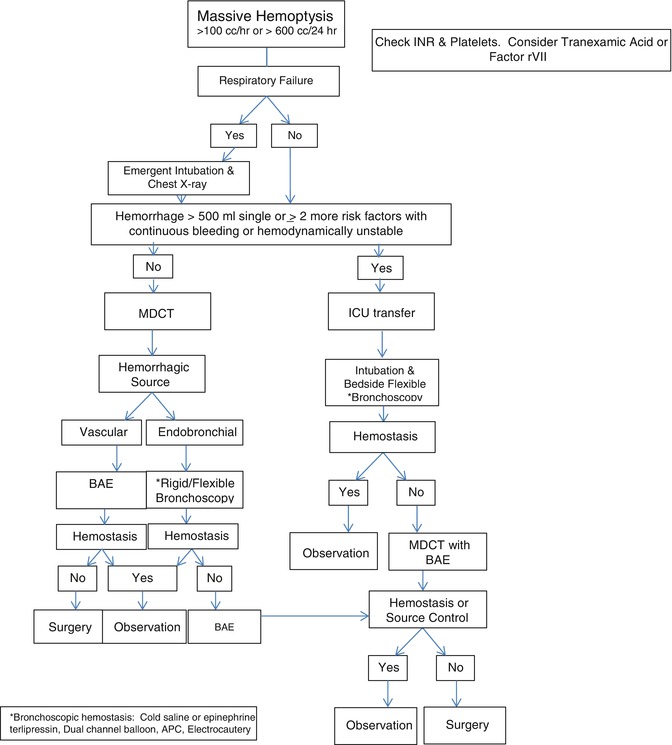
Fig. 26.4
Clinical algorithm to massive hemoptysis
Sources of Hemorrhage
Hemoptysis, including massive hemoptysis, usually originates from pathology that involves the high pressure bronchial arterial supply (90 %) [6, 7]. The bronchial artery or arteries originate from the descending thoracic aorta (DTA) at thoracic vertebral level T3-8 most often T5-6. While the most common pattern is a right and left bronchial artery arising from the DTA, variability is extensive, and commonly involves a right bronchial artery arising from an intercostal artery (also-called intercostobronchial trunk) or 2 right bronchial arteries arising from the DTA and/or intercostobronchial trunk. Left bronchial arteries can also arise from intercostobronchial trunks [7]. The spinal artery of Adamkiewicz supplies the distal thoracic and lumbar spinal cord and originates from an intercostal artery at thoracic vertebral level T9-12 in 75 % of patients. However, it infrequently originates between T5-T8 and may be occluded during embolization of the bronchial artery resulting in spinal cord ischemia or infarction [8].
The pulmonary artery infrequently is the source of hemoptysis. Infection, malignant disease, traumatic injuries (e.g. Swan Ganz catheter balloon rupture of PA) and arteriovenous malformations are the most common causes for pulmonary arterial bleeding [6, 9–11]. Rarely hemoptysis may involve non-bronchial or pulmonary arteries. Non-bronchopulmonary arteries may enter the lung via transpleural adhesions as a result of chronic inflammation or congenital anomalies and may anastomose with the pulmonary artery circulation [9, 10]. Other potential nonbronchial arterial sources include the aorta (ruptured aneurysm), intercostal arteries, coronary, thyrocervical, pericardiodiaphragmatic, musculophrenic, and inferior phrenic arteries. Diffuse alveolar hemorrhage syndromes are rarely a cause of massive hemoptysis.
Diseases Associated with Massive Hemoptysis
Many diseases have been associated with massive hemoptysis and vary by geographic region. Tuberculosis continues to be a major cause of massive hemoptysis world-wide. Bronchiectasis, malignancy, trauma, pneumonia, and mycetoma are the most causes of massive hemoptysis in the USA [12, 13] (Table 26.1).
Table 26.1
Causes of massive hemoptysis
Infectious | Mycobacterial (TB), Fungal (mycetoma), Necrotizing Bacterial Pneumonia (Klebsiella, Streptococcus, Staphylcoccus, Actinomyces) |
|---|---|
Neoplastic | Bronchogenic, Renal cell, melanoma, carcinoid, adenocystic, etc. |
Vascular | Bronchial artery aneurysm, Pulmonary artery aneurysm, Cardiac and Pulmonary Malformations, Arteriovenous malformations, Airway vascular fistula, Dieulofoy’s Disease, etc. |
Pulmonary | Bronchiectasis, Broncholithiasis, Diffuse alveolar hemorrhage, Crytogenic, Inhalation: crackcocaine, etc. |
Diffuse Alveolar Hemorrhage Syndromes | Granulomatosis with Polyangitis, Microscopic polyangitis, Anti-GBM (Goodpastures), Isolated pulmonary capillaritis, SLE, Eosinophilic granulomatosis with polyangitis, Antiphospholipid antibody, toxin and drug induced lung injury, IgA deposition vasculitis, etc. |
Trauma | High dose brachytherapy, Pulmonary artery rupture, Biopsy and Trauma |
Hematologic | Coagulopathy and Platelet disorders |
The etiology for hemoptysis will direct treatment decisions. Systemic diseases such as vasculitis will require anti-inflammatory or immunosuppression whereas coagulopathies will require reversal of coagulation abnormalities [13–19]. Focal lung or bronchial conditions causing massive hemoptysis may require either bronchoscopic intervention or bronchial artery embolization (BAE) as a first approach.
Imaging
Plain radiographs will not permit localization of bleeding site in upwards of 35 % of patients [20]. Multidetector CT angiography is capable of ascertaining the site of bleeding and/or suggesting a diagnosis in more than 80 % of patients and the yield may be higher with the use of reformatted image techniques [21]. Further, CT angiography is helpful to guide bronchial artery embolization [6, 7, 9, 20].
An Approach to Managing Life Threatening Hemoptysis (Algorithm, Fig. 26.4)
Several algorithms have been developed to provide guidance for an approach to severe or massive hemoptysis and most agree that an initial multidisciplinary approach is indicated with immediate evaluation by pulmonology, interventional radiology and thoracic surgery [22–25]. We propose the following:
The initial survey should include a simple “ABC” assessment: Airway, Blood loss, and Clinical condition.
Airway: Does the volume of bleeding into the airway require emergent airway management?
Blood: Has there been a single bleeding event of large volume >100 cc or is the bleeding recurrent? Is the bleeding in excess of 100 per hour for >2 h?
Clinical Condition: Is there hemodynamic instability (signs of hypoperfusion, tachycardia, or hypotension)?
The decision regarding immediate airway management should be determined. Adequate intravenous access should be established with at least two large bore IV lines. Fluid resuscitation should be initiated, if indicated. A complete blood count, testing for coagulopathies, and cross match for transfusion should be obtained. In addition, perform electrocardiogram and obtain cardiac biomarkers.
Intubation: Options are dual lumen or single lumen endotracheal tube with the intent to protect the lung on the non-bleeding side. Single lumen endotracheal intubation is preferred when airway visibility is poor (see discussion of dual lumen endotracheal tubes below).
Position: The patient should be positioned with the presumed side of bleeding dependent (lateral decubitus) to reduce the likelihood of flooding of the unaffected lung with blood. However, lateral decubitus position with the bleeding side down may worsen hypoxemia (due to increased perfusion to poorly aerated lung) [26].
Assessment
Active Hemorrhage and unstable: If transport is not considered safe, the initial evaluation to localize and treat would be with rigid and/or flexible bronchoscope. This may allow therapeutic endoscopic intervention (Cold Saline/ epinephrine [EPI], anti-diuretic hormone [ADH], argon plasma coagulation [APC], tamponade endobronchial blocker). (Table 26.2) [27, 30–33].
Table 26.2
Bronchoscopic and systemic treatments for massive hemoptysis
Treatment
Mechanism of action
Procedure
Complications
Cold Saline
Vasoconstriction with localized thrombosis
50 cc aliquots at 4 °C
Topical Epinephrine (Epi), terlipressin or ornipressinRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access





