23 Management of Gastrointestinal Bleeding
The incidence of upper GI bleeding is estimated to be 37 to 172 per 10,000 population per year. Upper GI bleeding is nearly twice as common in males as in females, and its incidence increases with age, a pattern that has been attributed to increased incidence of predisposing comorbid conditions.1,2 The mortality rate for patients with upper GI bleeding has remained relatively stable over the past 40 years, ranging from 3% to 14%.1 The risk of death depends on the patient’s age, presence of shock, comorbid medical conditions, presence of recent hemorrhage, location of the onset of bleeding (inpatient versus outpatient), and underlying cause of the hemorrhage (Table 23-1). Scoring systems to predict mortality and risk of rebleeding are based on host factors, the patient’s clinical course, and endoscopic findings.1,2 Variceal hemorrhage is associated with a mortality rate of 15% to 20%, and the risk of recurrent bleeding is about 30%.3,4
TABLE 23-1 Risk Factors for Death After Hospital Admission for Acute Upper Gastrointestinal Hemorrhage
Endoscopic findings (active, spurting hemorrhage from peptic ulcer; nonbleeding visible blood vessel; large varices with red spots) |
 Causes of Upper Gastrointestinal Bleeding
Causes of Upper Gastrointestinal Bleeding Causes of Lower Gastrointestinal Bleeding
Causes of Lower Gastrointestinal Bleeding
The most common cause of bleeding in patients younger than 50 years of age is hemorrhoids.5
 Major Causes of Gastrointestinal Bleeding
Major Causes of Gastrointestinal Bleeding
Peptic Ulcer Disease
Peptic ulcer disease accounts for as many as half of the cases of upper GI bleeding. It is also the most common cause of bleeding in patients with portal hypertension and varices.1 Bleeding from mucosal ulceration adjacent to a vessel can result from a Helicobacter pylori infection, use of nonsteroidal antiinflammatory drugs (NSAIDs), and/or critical illness. Concurrent aspirin and oral anticoagulation use further increases the risk of bleeding.6–9 Acid suppression therapy (H2-antagonists, proton pump inhibitors), however, has not affected the predominance of peptic ulcer bleeding as the cause of acute hemorrhage.10
Esophageal Varices
Gastroesophageal variceal hemorrhage is a major complication of portal hypertension from cirrhosis and accounts for 5% to 15% of all cases of bleeding from the upper GI tract.11–14 The most common site of varices is the distal 2 to 5 cm of the esophagus. Superficial veins in this anatomic region lack support from surrounding tissues (Figure 23-1).15 The dilation of distal esophageal varices depends on a threshold pressure gradient, most commonly measured by the hepatic venous pressure gradient, defined as the difference between the wedged, or occluded, hepatic venous pressure and the free hepatic venous pressure (normal gradient < 5 mm Hg). If the hepatic venous pressure gradient is below 12 mm Hg, varices do not form.16,17 Varices do not invariably develop in patients with gradients ≥12 mm Hg, so this pressure gradient is necessary but may not be sufficient in and of itself for varix formation.16,17 Gastroesophageal varices are present in 40% to 60% of patients with cirrhosis; their presence and size are related to the underlying cause, duration, and severity of cirrhosis.18

Esophagitis
Significant bleeding from esophagitis and erosive disease is the second most common cause of upper GI hemorrhage, often causing occult blood loss rather than acute bleeding.6–9 Clinically obvious bleeding is most likely in patients with extensive ulcerative disease or with an underlying coagulopathy.
Mallory-Weiss Tear
Mallory-Weiss tears usually occur in gastric mucosa, although 10% to 20% occur in esophageal mucosa. They account for approximately 5% to 7% of cases of upper GI hemorrhage.6–9 A history of retching is obtained in less than one third of patients.19 Bleeding from Mallory-Weiss tears remits spontaneously in most patients; 5% experience rebleeding. Patients who experience rebleeding from a Mallory-Weiss tear usually have an underlying bleeding diathesis.20,21
Diverticulosis
The prevalence of diverticular disease is age dependent, increasing from less than 5% at age 40 to 30% by age 60, to 65% by age 85. The high prevalence of the disease explains why diverticulosis is the most common cause of lower GI bleeding even though fewer than 15% of patients with diverticulosis develop significant diverticular bleeding. Diverticular bleeding typically occurs in the absence of diverticulitis, and the risk of bleeding is not further increased if diverticulitis is present.22 Risk factors for diverticular bleeding include23:
Neoplasms
Colon cancer is a relatively less common but serious cause of hematochezia. Neoplasms are responsible for approximately 10% of cases of rectal bleeding in patients older than 50 years, but neoplasms are rarely implicated as the etiology for GI bleeding in younger individuals.24 Bleeding occurs as the result of erosion or ulceration of the overlying mucosa. The bleeding tends to be low grade and recurrent. Bright red blood suggests left-sided lesions; right-sided lesions can manifest with maroon blood or melena.
Hemorrhoids
Hemorrhoidal bleeding typically is painless, often presenting as bright red blood on stools, in the toilet, or on toilet paper. Hemorrhoids are dilated submucosal veins in the anus, located above (internal) or below (external) the dentate line.25 They usually are asymptomatic but can manifest with hematochezia, thrombosis, strangulation, or pruritus. Hematochezia results from rupture of internal hemorrhoids that are supplied by the superior and middle hemorrhoidal arteries.
 Initial Management of Gastrointestinal Bleeding
Initial Management of Gastrointestinal Bleeding
Bleeding stops spontaneously in most patients, but aggressive management is required when bleeding does not quickly resolve or when patients are at high risk for rebleeding. Priorities include achieving hemodynamic stability and preventing complications such as pulmonary aspiration.26,27 The rate of bleeding dictates the urgency of management:
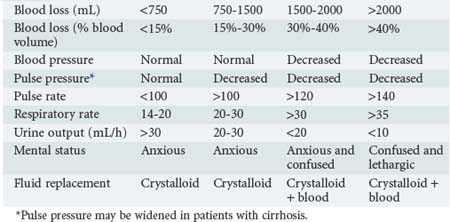
The degree of blood loss also can be estimated clinically by an evaluation of the heart rate, blood pressure, respiratory rate, urine output, and mental status (Table 23-2). The clinical estimation of blood loss is somewhat more difficult in patients with cirrhosis who have hyperdynamic circulation at baseline and a lower-than-normal systolic blood pressure and widened pulse pressure.
History and Examination
The clinical features of the GI bleeding provide clues to the probable source of bleeding within the GI tract (Table 23-3). When small amounts of bright red blood are passed per rectum, the lower GI tract can be assumed to be the source. In patients with large-volume maroon stools, aspiration via a nasogastric tube should be performed to assess the possibility of upper GI bleeding. Examination of nasogastric aspirate has diagnostic value, although in approximately 15% of patients with upper GI bleeding, the nasogastric aspirate fails to reveals blood or “coffee ground” material.26,27
TABLE 23-3 Clinical Indicators of Gastrointestinal Bleeding and the Probable Source Location Within the Gastrointestinal Tract
| Clinical Indicator | Probability of Upper Gastrointestinal Source | Probability of Lower Gastrointestinal Source |
|---|---|---|
| Hematemesis | Almost certain | Rare |
| Melena | Probable | Rare |
| Hematochezia | Possible | Probable |
| Blood-streaked stool | Rare | Almost certain |
| Occult blood in stool | Possible | Possible |
All patients with upper GI bleeding should have a nasogastric tube placed. Iced-saline lavage does not prevent or decrease upper GI bleeding.28 Gastric lavage with lukewarm tap water offers an equally safe and cost-effective alternative.29 Coffee-ground material or a frankly bloody gastric aspirate confirms an upper GI source of bleeding, whereas a nonbloody yellow-green nasogastric aspirate that contains duodenal secretions suggests the absence of bleeding proximal to the ligament of Treitz.30 However, in up to 50% of patients with a bleeding duodenal ulcer, a nonbloody gastric aspirate is obtained,29 possibly because of insufficient reflux of blood from the duodenum through the pylorus. Similarly, an intermittently bleeding upper GI lesion may result in a nonbloody gastric aspirate. The color of the gastric aspirate is of prognostic significance. Patients with coffee-ground or black gastric aspirates and whose stool is melanotic have a reported mortality rate of 9%.30 However, patients who have bright red blood per gastric aspirate and red blood per rectum have a 30% mortality rate.30 Red blood per rectum from an upper GI source usually signifies rapid bleeding.31
After the gastric contents have been aspirated, the nasogastric tube should be left in place to monitor ongoing bleeding and prevent pulmonary aspiration until there is no longer any evidence of bleeding. Maintaining this tube for a prolonged period, especially when the tube is attached to suction, may injure gastric mucosa and exacerbate GI hemorrhage.32
Initial Resuscitation
Volume resuscitation with crystalloids is the first priority in the management of any patient with GI bleeding. Two large-bore peripheral intravenous (IV) catheters should be inserted and/or a large-bore central line venous catheter should be established. Resuscitation should be initiated with crystalloid solutions, either normal saline (2 L) or lactated Ringer’s solution. Large-volume resuscitation with normal saline alone may cause a hyperchloremic metabolic acidosis and is possibly associated with coagulation abnormalities. Colloidal solutions have no role in the management of patients with acute GI bleeding. A complete blood count including platelet count should be obtained. Other key laboratory studies should include blood typing and cross-matching, prothrombin time (or international normalized ratio), activated partial thromboplastin time, blood chemistry panel, liver function panel. Transfusion of packed red blood cells should be initiated for patients with an estimated blood loss greater than 15%. Transfusion of fresh frozen plasma should be initiated for patients with preexisting coagulopathy (from liver disease or anticoagulation; see Table 23-2). Platelet transfusion is indicated if the platelet count is less than 50,000/µL.
The endpoints of resuscitation include normalization of heart rate, blood pressure, and indices of end-organ perfusion. Vasopressor agents initially should be avoided because pressor-mediated vasoconstriction in a hypovolemic patient can cause severe end-organ ischemia.33 Patients with a history of congestive heart failure, renal failure, or cirrhosis may require monitoring to assess cardiac parameters such as central venous pressure, cardiac output, stroke volume, and/or preload responsiveness. Although bedside pulmonary artery catheterization was widely used in the past for cardiac monitoring in the ICU, the recent trend in critical care medicine has been to use less invasive approaches such as bedside echocardiography or monitoring of pulse pressure variation.
Triage: Who to Admit to the Intensive Care Unit
The rate of rebleeding is approximately 3% in the low-risk group and 25% in the high-risk group. Patients in the low-risk group can be managed safely on a general medical floor. The decision regarding ICU admission should be individualized based on the patient’s risk stratification, age, comorbid diseases, clinical presentation, and endoscopic findings. Patients with active bleeding and two or more comorbidities have a mortality rate above 10% and should be observed in an ICU.34 Patients with coronary artery disease are best managed in an ICU because of the risk of myocardial ischemia secondary to hypovolemia and hypoperfusion.45 Admission to an ICU should be considered when endoscopic stigmata of recent hemorrhage, particularly visible vessels, are noted.
 Further Management of Upper Gastrointestinal Bleeding
Further Management of Upper Gastrointestinal Bleeding
Nonvariceal Bleeds
A meta-analysis of a large number of studies of nonvariceal bleeds demonstrated that endoscopic intervention decreased the mortality rate.35 Multiple endoscopic therapies, including injection of epinephrine, injection of alcohol, injection of thrombin, injection of fibrin glue, thermal contact, or application of hemostatic clips, have been evaluated. Monotherapy with epinephrine provides suboptimal hemostasis. However, epinephrine plus a second method significantly reduces the risk of rebleeding, surgery, or mortality.
Variceal Bleeding
Variceal bleeding stops spontaneously in more than half of patients; however, in those who continue to bleed, the mortality rate approaches 80%. Without treatment to obliterate the varices, there is a 60% to 70% risk of rebleeding. The risk for acute recurrent bleeding is highest within the first 72 hours of the initial bleed and decreases with time, similar to the case for peptic ulcer hemorrhage.36,37 Another option is variceal band ligation37,38; advantages over injection sclerotherapy include fewer local and systemic complications, lower rebleeding rates, fewer endoscopic treatment sessions to obliterate varices, and lower mortality rate.38–42
The diagnostic and therapeutic value of endoscopy in patients with upper GI bleeding is often limited by the presence of residual blood or clots.43 To avoid this problem, gastric lavage is usually performed with a large-diameter nasogastric tube just before endoscopy.44 Erythromycin induces rapid gastric emptying in healthy subjects and in patients with diabetic gastroparesis.44–46 Infusion of erythromycin (250 mg) just prior to endoscopy improves esophagogastroduodenal cleansing and enhances the quality of endoscopic findings.45
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


