7 Management of Cardiac Arrest and Post–Cardiac Arrest Syndrome
 Key Points
Key Points• The ultimate outcome of patients with cardiac arrest is frequently poor but can be improved by immediate bystander cardiopulmonary resuscitation, early defibrillation, and postresuscitation treatment.
• The classic ABC (airway, breathing, circulation) prioritization has changed to CAB to reinforce and prioritize early initiation of high-quality chest compressions and deemphasize early invasive airway management.
• Early defibrillation in patients with ventricular fibrillation and pulseless ventricular tachycardia is aided by various strategies, including automatic external defibrillators and improved provider awareness.
• Interruptions in chest compressions during cardiopulmonary resuscitation should be limited to maximize resuscitation; such interruptions can contribute to an unfavorable outcome.
• Postresuscitation care should include consideration of both induced hypothermia and urgent coronary reperfusion therapy.
Epidemiology
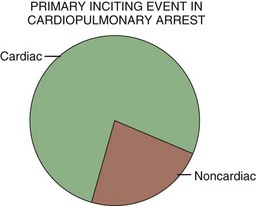
In the United States, sudden cardiac death accounts for approximately 200,000 to 500,000 deaths per year, with nearly half of these events occurring outside the hospital. Regarding the primary inciting event, cardiac causes of sudden cardiac death are most common (Fig. 7.1). Even though individuals with established cardiac disease have a greater than 50% incidence of sudden death, only a minority of cardiac arrest incidents occur in this population. It is estimated that half of all deaths from cardiovascular disease are sudden and unexpected and occur soon after the onset of symptoms. Patient age at the time of cardiac arrest has two distinct peaks—infants younger than 6 months and adults 45 to 75 years of age. Most sudden deaths occur outside the hospital and are often unwitnessed.1,2
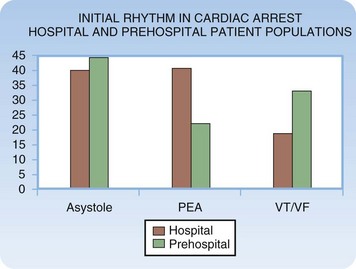
When resuscitation is successful, cardiac dysrhythmias remain a primary concern in the early phase of management of cardiac arrest. The four basic dysrhythmias encountered in cardiac arrest victims include pulseless ventricular tachycardia (VT), ventricular fibrillation (VF), asystole, and pulseless electrical activity (PEA). Pulseless VT and VF result in death unless treated aggressively and rapidly. Asystole, or effective absence of cardiac electrical activity, is the true cardiac arrhythmia (i.e., absence of any rhythm). PEA constitutes a diverse range of rhythms and related clinical scenarios. PEA is an electrical rhythm (i.e., the cardiac rhythm) with absence of discernible mechanical contraction of the heart and no detectable perfusion. The frequency of the dysrhythmias differs depending on the clinical setting (Fig. 7.2).
General Management Considerations
Resuscitation rates in patients with out-of-hospital and in-hospital cardiac arrest remain poor despite significant advances in the medical sciences. Contemporary research and recommendations have demonstrated that basic life support (BLS) interventions are very important therapies that have a positive impact on outcome.3 This same body of thought and investigation has suggested that advanced life support (ALS) treatments are of less value than originally thought.3 In addition, studies have demonstrated that early access to ALS treatment may be of less importance than previously believed.3,4 In the final phase of the Ontario Prehospital Advanced Life Support trial it was reported that in a community in which early CPR and early defibrillation are achieved, there is no survival benefit with the addition of prehospital ALS interventions.3 ALS is of value, but it is limited and less valuable than BLS measures in the early phase of most cardiac arrest events.
The 2010 guidelines of the American Heart Association (AHA) further deemphasizes advanced interventions. The 2010 AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care list five goals in the approach to cardiac arrest resuscitation: rapid activation of the emergency response team, effective and high-quality chest compressions, early access to defibrillation, effective ALS, and coordinated postresuscitation care.5 Only one of these five goals addresses ALS interventions.
Cardiopulmonary Resuscitation
Numerous investigations have demonstrated that chest compressions are delayed, frequently interrupted, and of poor quality. Wik et al found that CPR was performed only 48% of the time when indicated and that when it was performed, the mean rate was just 64 compressions per minute, with an appropriate depth (at least 5 cm) attained in only 28% of cases.6 Wang et al. and others reported that CPR was frequently interrupted for prolonged periods, anywhere from 1.8 to 7 minutes, to perform endotracheal intubation.7,8
One of the key components of the 2010 AHA guidelines5 is the change from performing the ABCs (airway, breathing, circulation) to the CABs,9 thus demonstrating how important compressions are relative to airway management and oxygenation—particularly early in cardiac arrest. Chest compression–only CPR has been proposed as an alternative method of basic resuscitation that is superior to traditional CPR with chest compressions and ventilations. The basic component of compression-only CPR is the performance of continuous, uninterrupted chest compressions of high quality. Compression-only CPR suggests that early management of the airway is not a priority.
Compression-only CPR has been shown to have similar efficacy to conventional CPR in terms of neurologically intact survival at 1 year in victims of witnessed cardiac arrest.10 In patients with an initially shockable rhythm, Kellum et al. demonstrated an increased survival rate with neurologically intact status after receiving compression-only CPR.11 The SOS-KANTO (Survey of Survivors After out-of Hospital Cardiac Arrest in the Kanto Area of Japan) trial reviewed 4068 patients with witnessed out-of-hospital cardiac arrests, 1151 of whom received bystander CPR. The 439 subjects who received hands-only CPR showed similar neurologic outcome at 30 days as did those who received conventional CPR (6% versus 4% of survivors); no benefit was seen with the addition of mouth-to-mouth ventilation.12 In 2008 using the concept of minimally interrupted cardiac resuscitation, Bobrow et al. demonstrated that cycles of 200 continuous compressions, followed by electrical defibrillation with immediate resumption of compressions before endotracheal intubation, resulted in an increased survival rate (1.8% versus 5.4%) in all patients. In the witnessed VF subgroup, the survival rate increased from 4.7% to 17.6%.13
Electrical Therapy
The most recent analysis of the timing of initial defibrillation suggests that there is no benefit with delayed defibrillation, even in patients with prolonged downtimes. Simpson et al. performed a meta-analysis of the existing literature and noted that no benefit was found in delaying the first shock in patients with prolonged downtimes or unwitnessed arrest (or both).14 The cumulative data demonstrated no benefit in providing chest compression before defibrillation versus immediate defibrillation and also no harm in performing CPR before the initial defibrillation. The 2010 AHA guidelines5,9 also acknowledged that the literature does not support a chest compression–first approach, thus suggesting that clinicians should provide both therapies (chest compression and defibrillation) and base the time of the first defibrillation on analysis of the setting, personnel, and equipment parameters for individual cases.
The other primary form of electrical therapy used in managing cardiac arrest is transcutaneous cardiac pacing. Very early use of transcutaneous ventricular pacing can be considered, although conclusive supporting evidence is lacking. Transcutaneous pacing is much less effective after the loss of spontaneous circulation or prolonged cardiac arrest.15,16 Transcutaneous pacing is a rapid, minimally invasive means of treating asystole and PEA bradyarrhythmias. Transcutaneous pacing electrodes are applied to the skin of the anterior and posterior chest walls, and pacing is initiated with a portable pulse generator. In an emergency situation, this type of pacing technique is easily and rapidly accomplished when compared with other methods of cardiac pacing.
Pharmacologic Therapy
Although numerous medications may be used in a resuscitation event, several “code drugs” are of potential importance, including epinephrine, vasopressin, atropine, amiodarone, lidocaine, magnesium, calcium, and sodium bicarbonate. Research into resuscitation after cardiac arrest has demonstrated that BLS interventions significantly contribute to favorable outcomes and that ALS treatments are less valuable than originally thought.3,17 A review of the issue has suggested that the use of cardioactive medications can increase the rate of successful resuscitation but does not alter the ultimate survival rate or have an impact on neurologic status at discharge among survivors.18
Atropine is a parasympatholytic drug that enhances both sinoatrial node automaticity and atrioventricular conduction via direct vagolytic action. In cardiac arrest, atropine can be considered in patients with both asystole and PEA, particularly those with bradydysrhythmic electrical activity. It is important to note that the AHA has removed atropine from all cardiac arrest algorithms.5,9 Removal of atropine is based not on any negative impact on patient outcome but on a significant lack of benefit.5,9 Atropine is still recommended in patients with compromising bradydysrhythmia with intact perfusion.5,9,19,20
Acute thrombosis with or without embolization, either coronary or pulmonary, can cause cardiac arrest. Many investigators have considered the early use of fibrinolytic agents in the management of cardiac arrest with known or presumed acute thrombosis. Anecdotal reports describe the cases of adult patients who have been successfully resuscitated following the administration of a fibrinolytic agent when the condition leading to the arrest was acute myocardial infarction (AMI) or acute pulmonary embolism.21 The 2010 AHA guidelines state that the evidence is insufficient to advocate the routine use of fibrinolytic agents during cardiac arrest but that its use should be considered on a case-by-case basis. Fibrinolytic agents are a level IIb recommendation in cardiac arrest secondary to pulmonary embolism.5,9
The Airway
The AHA has moved away from the airway-first strategy with a reordering of the resuscitation alphabet from the ABCs to the CABs, thus highlighting the relative importance of circulation over airway management.5,9 This change in strategy is based on the relative importance of circulation but also on the fact that airway interventions, particularly placement of an invasive airway, can interrupt continuous chest compressions and lessen the central nervous system (CNS), cardiac, and systemic perfusion produced by CPR. The airway should be managed invasively once appropriate chest compressions have been initiated and sustained and defibrillation has taken place. Management of the airway must not hinder appropriate chest compressions and other basic interventions. In cardiac arrest scenarios caused by a compromised airway or inadequate oxygenation and ventilation, or both, attention to invasive management of the airway is important.
Management of Specific Dysrhythmias
Ventricular Fibrillation and Pulseless Ventricular Tachycardia
Clinical Presentation
Ventricular Fibrillation
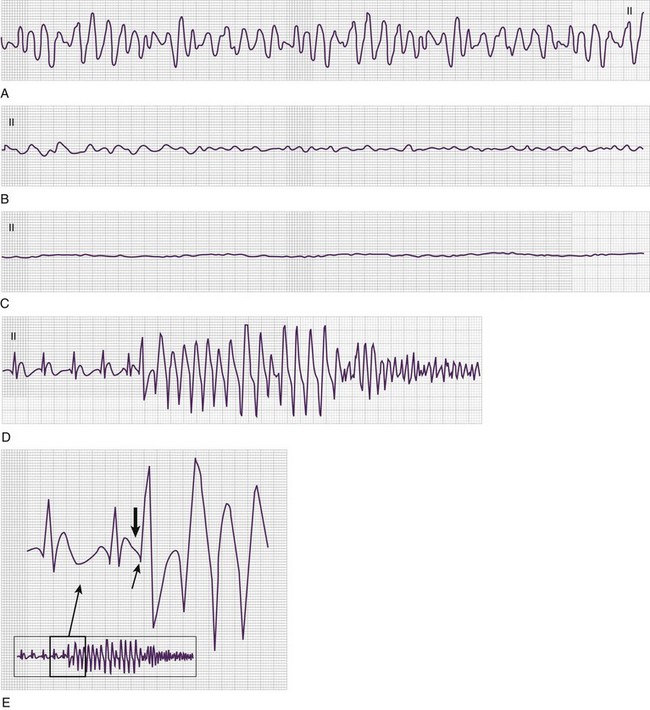
VF results in a lack of spontaneous perfusion except in the rare case of a witnessed, recent onset in which the patient is able to cough, thereby enabling perfusion to continue for a short period. VF is diagnosed electrocardiographically (Fig. 7.3) in pulseless and apneic patients by the presence of lower amplitude and chaotic activity. The rate of the deflections is usually between 200 and 500 depolarizations per minute. Morphologically, VF is divided into coarse (Fig. 7.3, A) and fine (Fig. 7.3, B and C). Coarse VF tends to occur early after cardiac arrest; is characterized by high-amplitude, or coarse, waveforms; and has a better prognosis than fine VF does. With continued cardiac arrest the amplitude dampens, with a less dramatic appearance of the dysrhythmia and fine VF (Fig. 7.3, B and C) ultimately being produced. The R-on-T phenomenon can result in VF as noted in Figure 7.3, D and E.
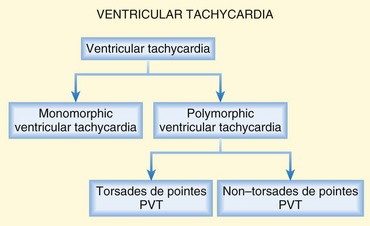
Ventricular Tachycardia
VT is defined as three or more ventricular beats in succession with a QRS complex duration of greater than 0.12 second and a ventricular rate greater than 100 or 120 beats/min (Fig. 7.4). Most instances of VT are characterized by very rapid rates; however, patients may have slower versions of VT, particularly if using amiodarone.