50 Lung Infections
 Key Points
Key Points• A wide variety of infectious agents, including bacteria, viruses, and fungi, cause pneumonia.
• Diagnosis and treatment of pneumonia are determined by assessment of patient risk factors, other elements of the history, diagnostic studies, and physical examination.
• Special care must be taken to identify patients at risk for health care–associated pneumonia or unusual or resistant organisms.
• Chest radiography is an important diagnostic tool that can offer valuable clues to the etiology. Other laboratory and sputum studies may also be useful.
• Because the causative agent is typically not known at initial evaluation, timely institution of carefully selected empiric antibiotic therapy is paramount.
• Age, comorbid diseases, and clinical and laboratory data guide disposition decisions for a patient with pneumonia, such as admission to an intensive care unit.
• Isolation measures such as droplet precautions should be initiated immediately for patients with acute febrile respiratory illnesses.
Epidemiology
Pneumonia is one of the most common infectious diseases encountered in the emergency department (ED), with more than 1.5 million visits for this infection annually.1 When combined with influenza, pneumonia ranks as the sixth leading cause of death in the United States and the most common cause of infection-related mortality.2–5
Pathophysiology
Pneumonia typically occurs when the protective defenses just described are breached and the lungs are exposed to a heavy inoculation of organisms or to very virulent organisms. The lung’s defenses can be impaired at multiple levels. Aspiration can result when altered levels of consciousness secondary to a neurologic insult or alcohol or drug intoxication impair the gag reflex. The upper airway defenses are often bypassed by endotracheal tubes or tracheostomy. Smoking and chronic lung disease can impair mucociliary function. Bronchial obstruction secondary to tumor or lymphadenopathy can lead to obstruction and pneumonia. Immunologic impairment as a result of infection with human immunodeficiency virus (HIV), chemotherapy, splenectomy, or advanced age also predisposes to pneumonia. The elderly are particularly vulnerable because of impairments at many of these levels and a higher incidence of comorbid conditions5 (Fig. 50.1).
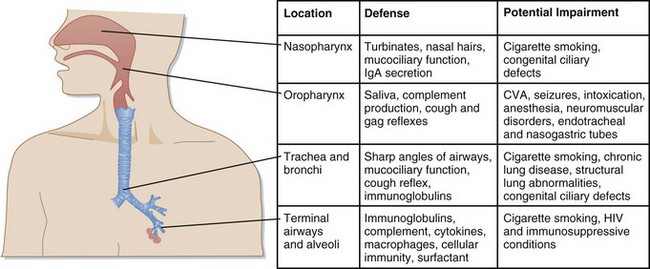
Fig. 50.1 Host defenses against infection.
CVA, Cerebrovascular accident; HIV, human immunodeficiency virus; IgA, immunoglobulin A.
(Modified from Donowitz G, Mandell G. Acute pneumonia. In: Mandell GL, Bennett JE, Doline R, editors. Mandell, Douglas, and Bennett’s principles and practice of infectious disease. 6th ed. Philadelphia: Saunders; 2005. pp. 819-41.)
Presenting Signs and Symptoms
A goal-directed, comprehensive history is very important in the evaluation of a patient with pneumonia. Historical clues such as risk for aspiration, recent travel, animal or environmental exposure, HIV status or risk, alcoholism, and comorbid illnesses can point toward specific causes and guide the proper choice of initial empiric therapy (Table 50.1).6,7 Special care should be taken to identify patients at risk for health care–associated pneumonia (HCAP), such as recent health care and antibiotic exposure, which could predispose them to multidrug-resistant pathogens and alter treatment choices.8
Table 50.1 Epidemiologic Conditions Related to Specific Pathogens in Patients with Selected Community-Acquired Pneumonia
| CONDITION | COMMONLY ENCOUNTERED PATHOGENS |
|---|---|
| Alcoholism | Streptococcus pneumoniae, oral anaerobes |
| Chronic obstructive pulmonary disease and/or smoking | S. pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Legionella spp., Chlamydia pneumoniae |
| Poor dental hygiene | Oral anaerobes |
| Aspiration/lung abscess | Oral anaerobes |
| Exposure to bats or to soil enriched with bird droppings | Histoplasma capsulatum |
| Exposure to birds | Chlamydia psittaci, avian influenza (poultry exposure) |
| Exposure to rabbits | Francisella tularensis |
| Exposure to farm animals or parturient cats | Coxiella burnetii (Q fever) |
| Human immunodeficiency virus infection: | |
| Early | S. pneumoniae, H. influenzae, Mycobacterium tuberculosis |
| Late | Above plus Pneumocystis jiroveci (carinii), Cryptococcus, Histoplasma |
| Travel to or residence in the southwestern United States | Coccidioides spp. |
| Travel to or residence in Asia | Burkholderia pseudomallei, severe acute respiratory syndrome |
| Influenza active in the community (“flu season”) | Influenza, S. pneumoniae, Staphylococcus aureus, H. influenzae |
| Structural lung disease (e.g., bronchiectasis) | Pseudomonas aeruginosa, Burkholderia cepacia, S. aureus |
| Injection drug use | S. aureus, skin anaerobes, M. tuberculosis, S. pneumoniae |
| Endobronchial obstruction | Anaerobes, S. pneumoniae, H. influenzae, S. aureus |
| Recent hospitalization or nursing home residence | Drug-resistant S. pneumoniae, gram-negative bacilli, S. aureus |
| In the context of bioterrorism | Bacillus anthracis (anthrax), Yersinia pestis (plague), F. tularensis (tularemia) |
Modified from File T, Niederman M. Antimicrobial therapy of community-acquired pneumonia. Infect Dis Clin North Am 2004;18:993-1016.
 Red Flags
Red Flags
Look for key clues in the history and physical findings that would suggest pneumonia caused by an unusual or resistant organism.
Identify patients at risk for health care–associated pneumonia.
Maintain high suspicion for aspiration pneumonia in the elderly and in patients with altered mental status or a recent cerebrovascular accident.
Pathogens
Community-acquired pneumonia is often defined as pneumonia in a patient who has not been hospitalized and has not resided in a long-term care facility for more than 14 days before the appearance of symptoms.3 With the growing prevalence of mixed-organism infections, drug-resistant pathogens, and patients with comorbid illnesses, this definition has become somewhat more complicated. Guidelines from the American Thoracic Society (ATS), Centers for Disease Control and Prevention, and Infectious Diseases Society of America (IDSA) now address the treatment of patients at increased risk for pseudomonal infection, those with significant comorbid conditions, and those at risk for infection with drug-resistant Streptococcus pneumoniae.
The most common etiologic agent causing pneumonia is S. pneumoniae, which is responsible for about two thirds of all cases (Table 50.2).3 Other bacterial pathogens that are often isolated are Mycoplasma pneumoniae, Chlamydia pneumoniae, Haemophilus influenzae, and Legionella pneumophila (often called “the atypical organisms”). Community-acquired pneumonia is also caused by several viruses, including influenza, parainfluenza, and respiratory syncytial virus (RSV). Other pathogens, such as Pseudomonas aeruginosa, drug-resistant S. pneumonia, and methicillin-resistant Staphylococcus aureus (MRSA), should additionally be considered in patients who have had recent health care exposure or have recently taken broad-spectrum antibiotics. Multiple other organisms may be considered based on a history of specific exposures, travel, and lung or immunosuppressive diseases.
Table 50.2 Etiology of Community-Acquired Pneumonia
| PATHOGEN | PREVALANCE (%) |
|---|---|
| Streptococcus pneumoniae | 20-60 |
| Haemophilus influenzae | 3-10 |
| Staphylococcus aureus | 3-5 |
| Gram-negative bacilli | 3-10 |
| Miscellaneous (includes Moraxella catarrhalis, group A streptococci, and Neisseria meningitidis, each accounting for 1-2% of cases) | 3-5 |
| Legionella spp. | 2-8 |
| Mycoplasma pneumoniae | 1-6 |
| Chlamydia pneumoniae | 4-6 |
| Viruses | 2-15 |
| Aspiration | 6-10 |
From Niederman M. Review of treatment guidelines for community acquired pneumonia. Am J Med 2004;117;52S.
Special Populations
Children
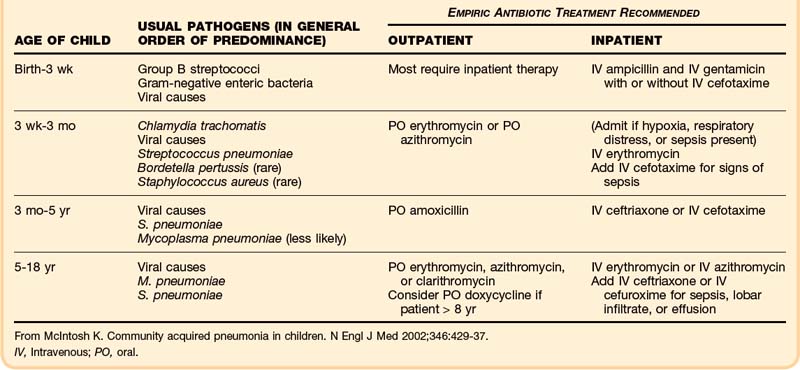
Pneumonia and acute bronchiolitis are the most common lower respiratory tract infections in children. They are caused by a variety of viruses and bacteria, with the prevalence varying by age group9,10 (Table 50.3). As in adults, S. pneumoniae is the predominant organism causing pneumonia except in newborns, in whom group B streptococci and gram-negative bacilli dominate. H. influenzae type b remains an important bacterial pathogen causing pneumonia in the developing world. It has nearly been eliminated in the United States through immunization practices. Pneumococcal vaccines also appear to be lowering the incidence of invasive pneumococcal disease and pneumonia, but more data are needed.11 Many viruses, mainly influenza, parainfluenza, and RSV, can also cause pneumonia in children. Most children with pneumonia have cough, fever, and abnormal lung findings. Signs of tachypnea and increased work of breathing are often present and may be the only signs of disease in infants.9
Pertussis (whooping cough) is a respiratory tract infection worthy of special mention. Caused by the organism Bordetella pertussis, it typically affects young children and adolescents. The incidence of the disease has markedly decreased because of immunization. Pertussis is manifested in three distinct stages. The first (catarrhal) stage consists of a mild cough, conjunctivitis, and coryza lasting up to 2 weeks. The second stage consists of severe paroxysms of coughing, often followed by strong inhalations of air, which produces the characteristic “whoop.” This stage can last up to 4 weeks. The third (convalescent) stage consists of a chronic cough. The disease is important to identify because multiple complications can occur, such as complete airway obstruction, secondary pneumonia, seizures, and encephalitis. Treatment is with oral erythromycin or azithromycin. Close contacts of the patient should receive prophylactic antibiotics.9
Patients Infected with Human Immunodeficiency Virus
Pneumonia is one of the most common serious bacterial illnesses affecting patients infected with HIV. In addition to the common community-acquired pathogens, patients with HIV are more susceptible to opportunistic infections with Pneumocystis carinii, pulmonary tuberculosis, and recurrent bacterial pneumonia. Antibiotic chemoprophylaxis, highly active antiretroviral therapy, and preventive vaccines appear to be significantly improving the incidence and the morbidity and mortality of pneumonia in patients with HIV.12
Aspiration Pneumonia
Aspiration of oral or gastric contents can occur in the setting of altered mental status or dysfunctional swallowing reflexes secondary to neurologic impairment such as stroke. Aspiration is typically “silent,” and therefore a high index of clinical suspicion is needed for making the proper diagnosis. Aspiration can lead to chemical pneumonitis and bacterial aspiration pneumonia more than 60% of the time.5




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


