Lumbar Plexus Blocks
A. Lumbar Plexus/Psoas Compartment Block
Rita Merman
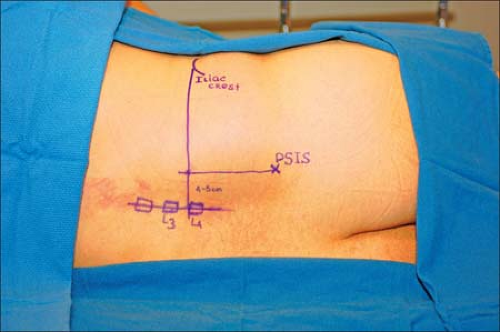 Figure 13-1. The intersection of the intercrestal line with the parasagittal line determines the site of introduction of the needle. Iliac Spine (IS). Postsuperior iliac spine (PSIS). |
The lumbar spine may be flexed as in the positioning for a lumbar epidural or spinal technique to help identify surface anatomy landmarks.
More cephalad approaches to the lumbar plexus should be avoided. With a more cephalad approach there is an increased risk of renal puncture and renal hematoma.

Figure 13-2. X-ray indicating appropriate positioning.

Figure 13-3. Evaluation of lumbar plexus blocks. Sensory innervation with ice. A: Femoral nerve. B: Lateral femoral cutaneous nerve. C: Obturator nerve.
One may elicit quadriceps muscle contraction, without hitting the transverse process.
If the stimulation of the femoral nerve in the lumbar plexus does not occur within 2 cm of the transverse process, the needle is withdrawn from the skin and reintroduced after increasing the needle angulations by 10° laterally.
If the transverse process is not contacted at a depth of 9 cm or deeper, and quadriceps contraction is not elicited, the needle should be withdrawn and redirected medially.
Hamstring contraction indicates stimulation of the L4 component of the sacral trunk at the level of the nerve root. The needle needs to be withdrawn from the skin and redirected laterally.
A scrotum/labial paresthesia indicates stimulation of genitofemoral nerve (L1 branch of lumbar plexus), which lies anteriomedial in the psoas compartment. The needle needs to be withdrawn from the skin and redirected more laterally and less caudally.
Stimulation of iliohypogastric nerve causes abdominal wall contraction. In this case, redirect the needle more medially.
Because of the risk of epidural spread, it is important to monitor blood pressure during the injection of local anesthetic to limit the epidural spread. A decrease in arterial blood pressure is the first symptom suggesting such diffusion.
Exercise caution with the needle depth to avoid intraperitoneal injection. Non-obese patients require a needle of no more than 100 mm in length, inserted to a depth of 70 to 90 mm. However, with morbidly obese patients the femoral nerve may be reached
at a depth of 150 mm. Even in these patients it is recommended to first start with a 100-mm needle, because there is no correlation between weight and the depth of the lumbar plexus.
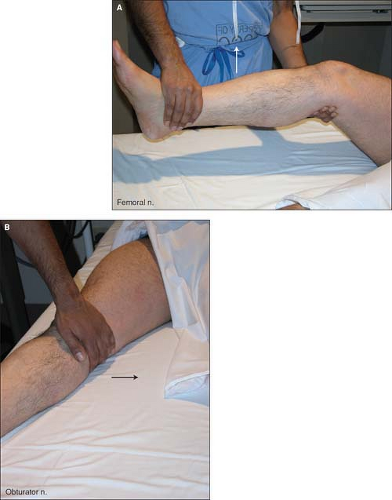
Figure 13-4. Evaluation of motor function against resistance. A: Femoral nerve. B: Obturator nerve.
The operator should ensure that a direct stimulation of the psoas muscle is not mistaken for a contraction of the quadriceps muscle by having an assistant place a hand on the quadriceps.
It is possible to identify the psoas compartment (a region containing the lumbar plexus) by using a loss-of-resistance approach. In fact, to reduce the number of punctures, it is possible to combine the use of the nerve stimulator and the loss-of-resistance approach by using an insulated needle connected to both a nerve stimulator (1.5 mA, 2Hz, 0.1 ms) and a loss-of-resistance syringe filled with 5 mL of air. As the needle goes through the posterior part of the psoas muscle a direct stimulation of the muscle is elicited. This muscle contraction disappears and a loss of resistance is felt when the needle enters the psoas compartment. After negative aspiration for blood, the local anesthetic solution can be injected slowly.
The aspiration of blood suggests the puncture of a paravertebral vein and indicates that the needle needs to be redirected laterally.
Local anesthesia is required to minimize patient discomfort using a 25-gauge, 38-mm needle and 5 mL of 1% lidocaine.
Moderate sedation should be provided in most cases with 1 to 2 mg of midazolam and 50 to 100 μg of fentanyl.
Suggested Readings
Aida S, Takahashi H, Shimoji K. Renal subcapsular hematoma after lumbar plexus block. Anesthesiology 1996;84:452–455.
Chayen D, Nathan H, Chayen M. The psoas compartment block. Anesthesiology 1976;45:95–99.
Ghisi AF, Matusic B, Joshi R, Chelly JE. Relationship between lumbar plexus and parasacral sciatic depth. Abstract. IARS 80th Clinical & Scientific Congress, 2006.
Mansour NY, Bennetts FE. An observational study of combined continuous lumbar plexus and single-shot sciatic nerve blocks for post-knee surgery analgesia. Reg Anesthes 1996;21:287–291.
Matheny JM, Hanks GA, Rung GW, et al. A comparison of patient-controlled analgesia and continuous lumbar plexus block after anterior cruciate ligament reconstruction. Arthroscopy 1993;9:87–90.
Muravchick S, Owens WD. An unusual complication of lumbosacral plexus block: a case report. Anesth Analges 1976;55:350–352.
Parkinson SK, Mueller JB, Little WL, et al. Extent of blockade with various approaches to the lumbar plexus. Anesth Analges 1989;68:243–248.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


