Cervical Blocks
Laurence Marr
General Comments
The regional approach to anesthesia for carotid endarterectomy offers several advantages over general anesthesia. With the patient awake, it offers an instant monitor of adequate blood flow from the contralateral side when the carotid artery is clamped. Additionally, hemodynamics are better preserved, compared with emergence from general anesthesia and extubation.
Cervical plexus block is an easy block to do in most patients, but there is a learning curve. As with most regional techniques, they are not always perfect, and it is important to have a plan to manage the failed blocks.
There are several points of note when doing regional anesthesia for carotid endarterectomy. First, it is important to choose patients who understand what is expected and explain the procedure well to them. They need to know they will be awake with little sedation, which means they will know they are being worked on and that they will feel touch, pressure, and temperature, but should be free from pain and discomfort for most of the procedure. Do not be afraid to change to a general anesthetic if when you begin the block the patient seems unduly uncomfortable with this approach. Second, it helps if the surgeon can complete the procedure in less than one and a half hours. Most of these patients are elderly and have arthritis, and will get uncomfortable if lying on a hard operating table for extended periods. Third, it is important that the surgeon be prepared to supplement the block with additional local anesthetic. There are two areas where this may be necessary. First, there are areas of overlap of unanesthetized dermatomes coming from the contralateral side, and because the incision comes close to the midline, it may be necessary to add additional local. Also, structures inside the carotid sheath receive innervation from the cranial nerves IX and X. If painful for the patient when the carotid sheath is entered, this can be eliminated by topical administration of local anesthetic to the area. If bradycardia becomes a problem with traction on the carotid sinus, then local anesthetic to that area can help. At the completion of the procedure and in the recovery room, it is important to control the blood pressure, as improved blood supply to the affected side can produce some mild cerebral edema and confusion if the blood pressure is too high.
Contraindications (absolute and relative)
Patient refusal
Patients that are confused and cannot cooperate
Patients with an uncontrollable cough
Patients that cannot lie flat
Patients with a high bifurcation of the common carotid requiring excessive retraction for surgical exposure
Anatomic Considerations
Anesthesia for carotid endarterectomy can be adequately supplied by blocking cervical nerves 2, 3 and 4. These nerves supply the area from behind the head down to the clavicle. Also, there is some overlap of dermatomes from the contralateral side. In addition, the third division of the trigeminal nerve supplies sensation down to the superior surface of the mandible. Lastly, the structures within the carotid sheath are supplied by cranial nerves IX and X.
The roots of the cervical nerves emerge superior to the transverse process of each cervical vertebra. The superficial plexus emerge form the border of the posterior border of the sternocleidomastoid muscle, the majority arising from the midpoint.
Supplies
Mayo stand and sterile cover
Three sterile towels
Prep solution
Cup for local anesthetic
Package of 4 × 4 sterile sponges
Three 5-cc syringes
One 10-cc syringe
Three 22-gauge × 1.5-in needles
One 25-gauge or smaller needle
One short extension tubing
One 20-cc vial of lidocaine 1.5% with 1/400,000 epi
One 20-cc vial of lidocaine 1% plain
Sedation
It is important not to oversedate the patient. The patient must be awake enough to follow commands, indicating adequate cerebral blood flow. A combination of benzodiazepines and narcotics can be titrated to a desired effect. In the elderly benzodiazepines may result in restlessness and confusion.
Technique
Step 1
The patient is placed on the table with the head slightly extended and turned to the contralateral side.
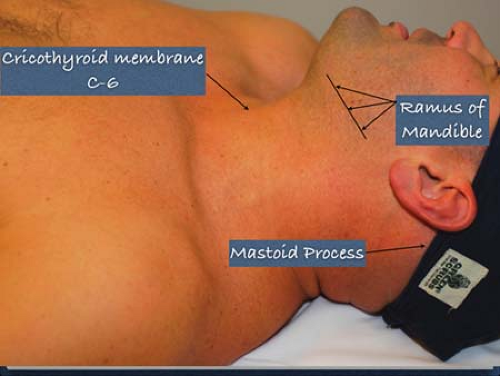 Figure 16-1. Anatomic landmarks. |
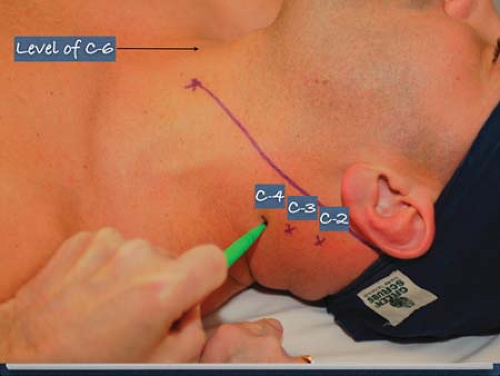 Figure 16-2. Location of C-2, C-3, and C-4. |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


