84 Knee and Lower Leg Injuries
 Key Points
Key Points• Knee dislocations are associated with a high risk for neurovascular injury and constitute an orthopedic emergency.
• A grossly unstable knee should be assumed to have been dislocated.
• Patients with fractures or dislocations of the knee and lower extremity and neurovascular compromise should undergo emergency reduction or realignment before any radiographic evaluation.
• Patients discharged home in knee immobilizers with stable injuries should be instructed to remove the device several times a day and perform range-of-motion and quadriceps-strengthening exercises.
• The cast or splint should be removed from any patient with increasing pain after a lower leg fracture to allow careful assessment of neurovascular status and evaluation of the lower leg compartments.
Pathophysiology
Knee
Anatomy
Knee stability is provided solely by ligaments and tendons in and around the joint (Fig. 84.1). The knee joint is encapsulated by fibrous connective tissue lined by a synovial membrane. The knee capsule is continuous with the suprapatellar bursa, which expands when a joint effusion is present.
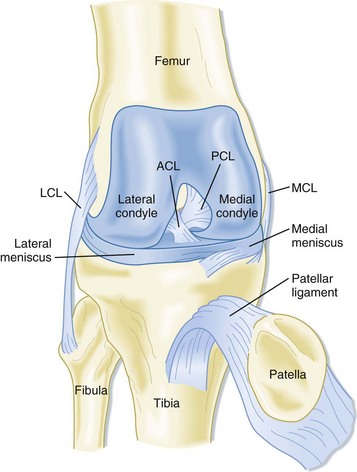
Fig. 84.1 Knee anatomy.
(From Brown JR, Trojian TH. Anterior and posterior cruciate ligament injuries. Prim Care 2004;31:925–56.)
Evaluation
Key aspects of evaluation of knee are listed in Box 84.1. In general, evaluation of knee complaints should also include an examination of the hip and back to prevent overlooking a source of pain referred to the lower extremity.
Box 84.1 Evaluation of the Knee
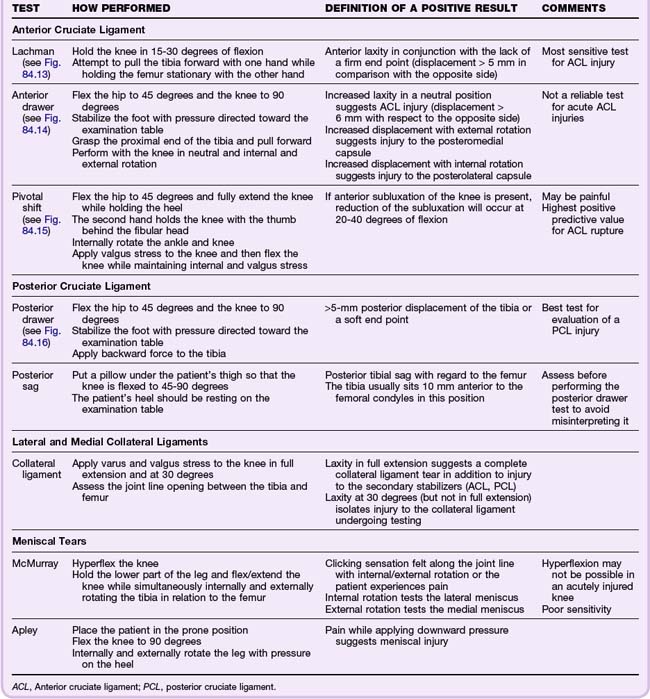
During evaluation, the point of maximal tenderness should be assessed last. Specific tests for evaluating ligamentous and meniscal injuries are detailed in Table 84.1. Comparison with the uninjured or normal knee is helpful, especially for assessment of ligamentous laxity.
Diagnostic Testing
Because acute injuries to the knee commonly involve soft tissue, plain radiographic examination is not always indicated. The Ottawa Knee Rules1 (Box 84.2) and the Pittsburgh Knee Rules2 (Box 84.3) are useful guides to aid in the decision of whether to order plain radiographs. Both criteria are sensitive for fractures, but the Pittsburgh criteria are more specific and can be applied to both children and adults.
Box 84.2 Ottawa Knee Rules
Radiographs indicated if any one of the following is present:
• Tenderness at the head of the fibula
• Isolated tenderness of the patella
• Inability to flex the knee to 90 degrees
• Inability to bear weight for four steps both immediately after the injury and in the emergency department
Box 84.3
Pittsburgh Knee Rules
• The patient is younger than 12 or older than 50 years.
• The patient is unable to walk four weight-bearing steps in the emergency department.
Data from Seaberg DC, Yealy DM, Lukens T, et al. Multicenter comparison of two clinical decision rules for the use of radiography in acute, high-risk knee injuries. Ann Emerg Med 1998;32:8–13.
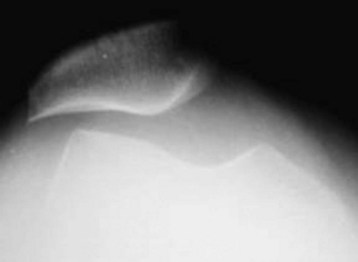
If plain radiographs are indicated, a minimum of an anteroposterior (AP) and a lateral view should be obtained. Oblique radiographs are helpful for detecting subtle tibial plateau fractures. The intercondylar or tunnel view is helpful in evaluating for tibial spine fractures and osteochondral defects (Fig. 84.2). Assessment of the patellofemoral joint and evaluation for the presence of patellar tilt (increased propensity for patellar subluxation or dislocation) can be done with the Merchant or sunrise view (Fig. 84.3). Comparison radiographs of the unaffected extremity are helpful in discerning problems in skeletally immature patients.

Fig. 84.2 Knee radiograph, tunnel or intercondylar view, showing an osteochondritis dissecans lesion (arrows).
When describing the knee radiograph, the examiner should note the alignment and joint spacing of the femoral condyles in relation to the tibial plateau. Narrowing of the joint space (particularly in weight-bearing views) indicates articular cartilaginous and meniscal degeneration. The patella should be examined for possible fractures (in the event of a direct blow to the anterior aspect of the knee) and the presence of a bipartite or tripartite patella. Significant joint effusions are evident as a water-density radiolucency on the lateral view, anterior to the distal end of the femur.3 Effusions seen shortly after injury are suggestive of anterior cruciate ligament (ACL) or posterior cruciate ligament (PCL) tears, tibial plateau fractures, femoral condyle fractures, or patellar fractures.4
In the setting of acute injuries, radiographs should be examined for the presence of fractures involving the tibial plateau (depression fracture) or tibial spine (suggesting rupture of the ACL). Segond fractures are avulsion fractures of the lateral tibial plateau at the site of attachment of the lateral capsular ligament. These fractures are associated with ACL and meniscal injuries. The presence of posterior opaque bodies should also be noted. These may be fabellae (congenital sesamoid) or loose bodies. More than 75% of loose bodies originate from osteochondral lesions.3 Occult fractures that are commonly missed on plain radiographs include patellar, tibial plateau, fibular head, and Segond fractures.5
Musculoskeletal ultrasound techniques can be used to diagnose ACL and PCL tears and may be helpful in the diagnosis of meniscal injuries.4 Magnetic resonance imaging (MRI) can be used to confirm suspected meniscal injuries, ligamentous disruptions, osteochondral lesions, and occult fractures; however, it is rarely indicated in the acute setting. Computed tomography (CT) is helpful for establishing the extent of certain fractures (e.g., tibial plateau fractures) and is often more readily available than MRI.
Lower Leg
Anatomy
The thigh muscles attach to the upper part of the tibia and lend stability to the knee joint. The muscles of the lower part of the leg, which are enclosed by fascia, can be divided into four compartments: anterior, posterior, deep posterior, and lateral (Fig. 84.4). Specific motor and sensory nerve distributions are listed by compartment in Table 84.2.
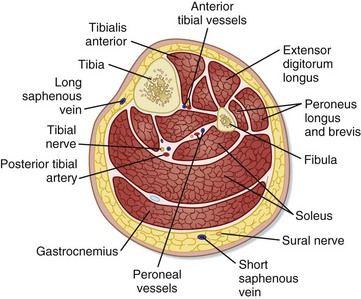
Fig. 84.4 Cross section of the lower extremity at the level of the calf.
(From Khatri VP, Asensio JA. Operative surgery manual. Philadelphia: Saunders; 2003.)

Dislocations and Fractures
Dislocations
Knee Dislocations
Knee dislocations are relatively uncommon and represent, at most, 0.2% of all orthopedic injuries. They require disruption of at least three of the four major ligaments of the knee. Common mechanisms include traffic accidents, sporting injuries, or simple mechanical falls. Dislocations are classified on the basis of the direction of tibial movement in relation to the femur. Anterior and posterior dislocations account for approximately 70% of all knee dislocations. Knee dislocations may also have associated intraarticular fractures involving the tibial plateau or femoral condyles.6
Knee dislocations are associated with a high risk for neurovascular injury and should be considered an orthopedic emergency. The neurovascular bundle runs posterior to the bony and ligamentous structures in the popliteal fossa. The popliteal artery and nerve are fixed in the fibrous tunnel of the adductor magnus muscle proximally and traverse the fibrous arch of the soleus muscle and interosseous membrane distally. The relative immobility of the neurovascular bundle makes it susceptible to injury. The popliteal artery may be injured in up to 14% of all knee dislocations (Fig. 84.5). Traction injuries to the common peroneal and, less commonly, to the tibial nerve may also be present.6

Neurovascular status should be documented before and after reduction. All patients with a suspected or confirmed knee dislocation should have the ankle-brachial index (ABI) calculated. An ABI of less than 0.9 has high predictive value for a vascular injury, and such patients should undergo either CT or traditional angiography. Patients with normal findings on vascular examination and an ABI lower than 0.9 should be observed for at least 24 hours with neurovascular checks every 2 to 3 hours.4 Prompt diagnosis of vascular injury is essential given the chance of development of progressive distal ischemia. When injury to the popliteal artery has occurred, patient outcome is directly related to the duration of ischemia.
Standard AP and lateral radiographs are adequate for initial evaluation of knee dislocations. After appropriate analgesia and sedation, emergency reduction of the dislocated knee should be attempted. Longitudinal traction on the tibia (to free it from the femur) should be followed with a force in the opposite direction of the dislocation. The rotary components should also be corrected to restore normal leg alignment. After reduction, the knee should be immobilized in 15 to 20 degrees of flexion.4 Orthopedic consultation in the ED is mandatory for all suspected and confirmed knee dislocations.
Patellar Dislocation
The patella normally articulates in the groove between the femoral condyles. The vastus medialis, medial and lateral patellofemoral, and patellotibial ligaments and the medial retinaculum all stabilize the patella (Fig. 84.6).
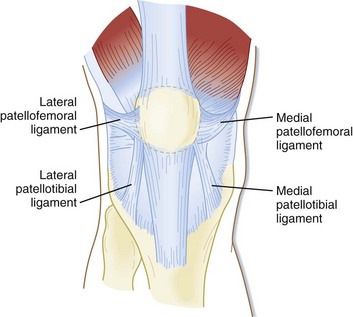
Fig. 84.6 Patellofemoral and patellotibial ligaments.
These structures act as static stabilizers of the patella.
(From DeLee JC, Drez Jr D, Miller MD. DeLee & Drez’s orthopaedic sports medicine: principles and practice. 2nd ed. Philadelphia: Saunders; 2003.)
The overall incidence of patellar dislocations is estimated to be 7 per 100,000 per year and as high as 31 per 100,000 per year in patients between the age of 10 and 19 years.7 Patellar dislocations most commonly occur when a varus force is applied to a flexed knee or after forced contraction of a flexed quadriceps. Dislocations may be associated with meniscal tears, disruption of the medial collateral ligament, and osteochondral fractures.4




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


