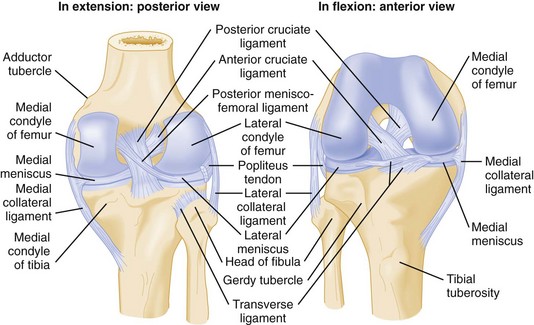
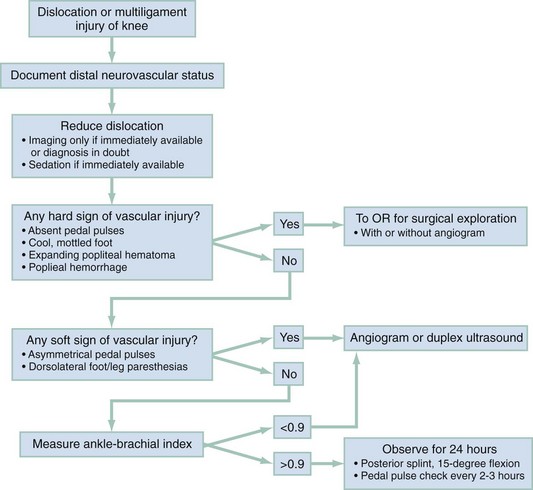
Chapter 57 More than 1 million knee injuries are treated annually in North American emergency departments (EDs).1 These injuries range in severity from minor contusions to limb-threatening injuries to the popliteal artery. The knee joins the longest mechanical levers in the body, the femur and tibia, and is therefore subject to high forces. It is the largest and most complex joint in the body and functions through a complicated interaction of flexion, extension, rotation, gliding, and rolling. Its large synovial space frequently is involved in infections and other inflammatory conditions. The knee is a modified-hinge diarthrodial synovial joint that consists of the tibiofemoral and patellofemoral joints.2 The head of the fibula, although not part of this articulation, is closely approximated laterally and provides a site for the attachment of muscles and ligaments. Joint stability is provided by ligaments, although surrounding muscles and the joint capsule contribute as well (Fig. 57-1). Depending on the population studied, management of knee and leg fractures commonly requires immobilization, which can result in deep vein thrombosis in up to 19% of patients. Prophylactic treatment with low-molecular-weight heparin reduces this risk.3 Dislocation is among the most serious of knee injuries, because the popliteal artery is commonly injured. Because many knee dislocations reduce spontaneously before the patient arrives at the ED, normal findings on physical examination and radiographs do not rule out a recent dislocation.4 If a history of knee dislocation is suspected or when a trauma patient has unexplained vascular insufficiency of the foot, thorough evaluation of the neurovascular status of the feet is an integral part of the secondary trauma survey. Proper examination of the knee requires the patient to be supine with both legs exposed. The question of whether knee pain may be the result of hip or spine pathology should be raised early, and the neurovascular integrity of the foot should be assessed. Examination of the knee begins with visual inspection (Box 57-1), followed by palpation (Fig. 57-2). Any obvious deformity, swelling, effusion, or ecchymosis is noted. Localized swelling should be distinguished from the presence of a joint effusion, which may obliterate the normal contour of the knee. If a large effusion is present, the patella is elevated from the femur by fluid, and the patella can be “ballotted” against the femur. Loss of the medial peripatellar concavity may be the only sign of a small knee effusion. A small knee effusion may be accentuated by milking the suprapatellar pouch inferiorly to force fluid into the knee joint. An effusion in the prepatellar bursa is found just beneath the skin anterior to the patella; this should not be confused with a knee effusion. Stability Testing: Although range of motion is important for documentation of disability, it is stability testing that provides the most specific diagnostic information. Stability testing seeks to identify tears of the four major ligaments of the knee—the ACL, PCL, MCL, and LCL. Stability testing in the acute phase is often misleading owing to splinting and effusion and is often not clinically useful in the ED. When the acute phase has passed, the goal of stability testing is to determine whether a patient may benefit from orthopedic referral for evaluation and repair. Anterior Drawer Test: The anterior drawer test seeks to identify tears of the ACL. A positive test result is defined as greater anterior movement of the tibia as compared with the other knee. The test is performed with the patient in a supine position, the hip flexed at 45 degrees, and the knee flexed at 90 degrees. The examiner may stabilize the patient’s tibia by sitting on the patient’s foot. The examiner then determines the amount of step-off between the femoral condyle and the tibial plateau by placing the thumbs over the joint line while exerting a smooth, gentle pull anteriorly on the tibia. The amount of forward displacement is compared with that on the normal side. Significant laxity relative to the contralateral knee is fairly specific for ACL disruption, although a false-positive result can be caused by PCL insufficiency, which allows the tibia to slip back on the femur, with anterior movement as the slack in the PCL is taken up. Sensitivity of the anterior drawer test is poor—10% acutely and only 50% with general anesthesia.5 False-negative findings may result from an effusion preventing knee flexion to 90 degrees, insufficient force applied during the test, or simply the strength of the knee flexors and extensors preventing abnormal movement. Lachman’s Test: Lachman’s test is the most accurate physical test for anterior cruciate ligament damage, with a sensitivity of 80% when performed acutely and 100% when performed with the patient under general anesthesia.5 Lachman’s test is done with the knee flexed 20 to 30 degrees while the examiner uses one hand to grasp the thigh and stabilize it. The tibia is pulled anteriorly, and the examiner notes tibial excursion. The examiner records “firmness” or a “soft endpoint.” The endpoint can be graded as 1+ (0-5 mm more displacement than on the normal side), 2+ (5-10 mm), or 3+ (more than 10 mm). The knee should be in a neutral position before manipulation, and the PCL must be intact for the test results to be valid. In an acute injury, any difference in translation or the feeling of a soft or indistinct endpoint may indicate a ligament tear. A PCL injury results in a false-positive test result as the knee is pulled forward. Potential causes of false-negative test results include hamstrings that are very strong or in spasm, meniscal tears, and third-degree MCL tears with posterior medial extension. Partial tears are not detected reliably. Lachman’s test is difficult if the examiner’s hands are small relative to the patient’s thigh. Pivot Shift Test: The pivot shift test, also called subluxation provocation or the jerk test, is performed to detect anterolateral rotatory instability associated with an injury to the ACL or lateral capsular structure. This test should be done carefully, if at all, in the acutely injured knee because the test maneuvers can exacerbate the initial injury. Sensitivity in the acute phase is only 27%, but the test is highly specific for ACL tear.6 Posterior Drawer Test: The posterior drawer test assesses for PCL injury.5 The posterior drawer test can be accomplished with the patient’s knee flexed at 90 degrees and the foot stabilized by the examiner’s thigh. A smooth backward force is applied to the tibia. Posterior displacement of the tibia more than 5 mm, or a “soft endpoint,” indicates injury to the PCL. A normal knee should exhibit no significant posterior excursion. The posterior drawer test result may be positive in only 85% of patients with PCL insufficiency documented operatively. Posterior Sag Sign Test: The posterior sag sign test is a second method of determining PCL integrity. Sensitivity in the acute phase is 79%.5 The test is done as follows. The patient is placed in a supine position, and a pillow is placed under the distal thigh for support while the heel rests on the stretcher. The knee is flexed to either 45 or 90 degrees, depending on which position provides the greater muscle relaxation. If the tibia sags backward, the test result is considered to be positive, indicating PCL insufficiency. If the posterior sag sign is not appreciated before the different drawer tests are performed, a false-positive result on the anterior drawer test is misinterpreted as an ACL injury. Posterior sag also may be shown by passive elevation of the leg in a fully extended position, with the examiner applying the elevating force at the ankle. As the leg is elevated, the tibia may fall back on the femur if the PCL is ruptured. Instrument Testing: Arthrometers are devices that quantitate anterior displacement of the tibia relative to the femur and are far more accurate in diagnosing ACL tears than the anterior drawer and Lachman’s tests, although these devices are rarely used in the ED setting. Studies in which commercially available arthrometers were used indicate that a side-to-side difference exceeding 3 mm of anterior displacement at 20 pounds is predictive of ACL injury with high accuracy.7 Collateral Ligament Stress Test: The collateral ligament stress test is used to test the integrity of the MCL and LCL. With the patient lying supine, the examiner applies varus and valgus stress with the knee at 0 and 30 degrees of flexion. Joint line opening is the amount of movement (i.e., hinging) produced between the tibia and the femur; this can be palpated and estimated in millimeters. The normal knee should be subjected to the same amount of valgus and varus stress, and the joint line opening is then compared with that in the injured knee. Isolated collateral ligament tears are detected only with the knee in slight flexion, because in extension the cruciate ligaments, capsule, and lesser ligaments of the knee provide significant lateral stability. Laxity in full extension implies complete collateral ligament tear and also injury to the cruciate ligaments or other structures. Laxity may be graded as follows: grade I, some laxity; grade II, marked laxity; and grade III, total laxity. Assessing for Meniscal Tears: Meniscal tears are difficult to diagnose in the acute setting, and these assessments are best reserved for the convalescent phase. Even then, small meniscal tears can cause significant symptoms but may not be detected on physical examination, and arthroscopic evaluation may be required for diagnosis. However, meniscal tears are likely to limit activity, rather than leading to further damage, so there is less urgency. By contrast, failure to diagnose a nondisplaced fracture can lead to displacement and severe consequences. McMurray’s Test.: McMurray’s test is used to help identify meniscal tears. The patient is placed in supine position with the knee hyperflexed. The examiner grasps the foot with one hand and the knee with the other. The examiner flexes and extends the knee while simultaneously internally and externally rotating the tibia on the femur and providing slight varus and valgus stress. A positive test result is the occurrence of clicking palpable along the joint line, or locking of the knee. Internal rotation of the leg tests the posterior segment of the lateral meniscus. External rotation tests the posterior segment of the medial meniscus. In the acute setting, limitation of range of motion may not allow sufficient hyperflexion to perform McMurray’s test, and the test result may be falsely negative. Apley’s Test.: Apley‘s test also aids in diagnosing meniscal tears. With the patient prone, the knee is flexed 90 degrees, and the leg is internally and externally rotated with pressure applied to the heel. Pain elicited by downward pressure suggests meniscal pathology. The pain should be relieved with distraction of the knee and rotation of the leg back to a neutral position. Although relatively specific, Apley’s test is not sensitive.6 Plain Radiographs: In acute knee trauma, the goal of radiography is to rule out fracture. Because radiographs are not 100% sensitive, knee immobilization and orthopedic referral for reevaluation are options. When suspicion for a fracture is extremely high, computed tomography (CT) can be used; it is more sensitive than plain films. One study found a negative predictive value of only 49% for plain films in diagnosing knee fracture, with CT as the gold standard.8 Magnetic resonance imaging (MRI) is even more sensitive but is not customarily used in the ED evaluation of knee and leg trauma. Plain films are useful for diagnosing fracture, effusion, foreign bodies, joint space narrowing, and lipohemarthrosis. Evaluating plain films begins with an assessment of bone anatomy and alignment. Nonobvious fractures are best detected by careful inspection of the cortex of all visualized bones. Any disruption of the continuous line of the cortex should raise suspicion for fracture. Subtle cortical disruptions indicate either nondisplaced fractures or draining cortical veins. The next step is to evaluate for the presence of an effusion, seen as a radiolucent area (of density similar to that of fat) distending the joint capsule. Presence of a linear interface between two different densities within an effusion suggests lipohemarthrosis (see Fig. 57-3), in which the effusion contains not only blood but also fat. This feature results from entry of marrow fat into the joint cavity and is diagnostic of fracture. The traditional practice was to obtain anteroposterior (AP) and lateral radiographic views of the knee in all cases of acute knee trauma. More recent work has led to validation of clinical decision rules that help decrease unnecessary radiography.9–11 The Ottawa Knee Rule states that radiography is necessary only if any one of five conditions is present: (1) age older than 55 years, (2) inability to transfer weight from one foot to the next four times at the time of injury and in the ED, (3) inability to flex the knee to 90 degrees, (4) patellar tenderness with no other bone tenderness, or (5) tenderness of the fibular head. Initial tests found that this rule detected 100% of fractures while allowing significantly fewer radiographs to be done.10,11 The Pittsburgh Knee Rule similarly was found to be 100% sensitive.12 This decision rule states that radiography is necessary only if the patient fell or sustained blunt trauma to the knee and if either of two conditions is present: (1) age younger than 12 or older than 50 years or (2) inability to walk four full weight-bearing steps in the ED. In a study comparing these two decision rules, both had good sensitivity, but the Pittsburgh rule was more specific, allowing fewer radiographs to be done without sacrificing sensitivity; in this study, the sensitivity of the Ottawa rule was 97% (95% confidence interval, 90 to 99%) and the sensitivity of the Pittsburgh rule was 99% (95% confidence interval, 94 to 100%).13 Either rule may be used, but patients should be told that this approach is associated with an approximately 1% chance of a missed fracture and that they should seek reevaluation in the event of persistent or progressive symptoms. One study validated the Ottawa Knee Rule in children older than 5 years, finding a sensitivity of 100%. The Ottawa Knee Rule permitted a 31% reduction in the number of radiographic evaluations.14 In another pediatric study of the Ottawa Knee Rule, 1 of 13 fractures was missed, implying a sensitivity of only 92%, so application of the rule in children still requires clinical judgment.15 In another approach, investigators asked whether a single lateral radiograph could replace the traditional three-view “knee series” (AP, lateral, and tunnel views). These investigators found that a single lateral view could detect 100% of fractures identifiable on the full series.16 This innovative approach merits further study. Computed Tomography: CT is most useful in detecting and classifying tibial plateau fractures and usually is done when the diagnosis is unclear or if operative intervention is being considered. CT angiography is an excellent tool for detecting injury to the popliteal artery, although its sensitivity relative to traditional angiography has not been quantified in large high-quality studies.17 In the ED evaluation of trauma to the knee and leg, angiography is used to seek popliteal artery injury after knee dislocation. To obtain an angiogram, a catheter is placed in the femoral artery and contrast is injected while fluoroscopy (video x-ray examination) is performed. Complications occur in about 1.7% of these procedures, and include vascular injury and contrast nephropathy. False-positive results can lead to unnecessary surgical exploration. From a practical standpoint, the patient must be removed from the ED to a radiology suite, where other injuries cannot be addressed, and the angiography team must be mobilized, often resulting in delays in care.4 Because of these limitations, relatively accurate alternatives, including CT angiography and duplex ultrasound, have been adopted.17 MRI is highly accurate for diagnosis of fractures and ligamentous injuries, although it often misses small meniscal tears. It has proved to be superior to other imaging modalities in the evaluation of osteonecrosis, osteochondritis dissecans, occult fractures, and bone contusion.18 Its advantages are that it is noninvasive and painless and does not involve exposure to ionizing radiation. MRI of the knee is rarely performed on an emergency basis, because immobilization and non–weight-bearing status are the usual procedure, pending outpatient orthopedic evaluation. Arthroscopy of the knee is the most commonly performed orthopedic surgical procedure in the United States. This nonemergent procedure is useful in diagnosis and treatment of knee injuries, including injuries of the meniscus, cruciate ligaments, articular cartilage, capsule, and synovium. The superior diagnostic accuracy of arthroscopy compared with the clinical knee examination has been well documented. In particular, arthroscopy has increased the accuracy of diagnosis of ACL injuries and small capsular tears. It is especially helpful in children, in whom diagnosis can be difficult because developing skeletal changes can obscure pathology. Difficulties in visualization arise when the capsular structures are tight and when meniscal tears are situated posteriorly. Arthroscopy is superior to MRI for diagnosis of meniscal tears and other soft tissue injuries, and the diagnosed problem can be repaired immediately. The need for arthroscopy is established in the convalescent phase of injury and need not be determined in the emergent setting, so long as appropriate referral to an orthopedist is made.19 An open joint is considered a surgical emergency. When violation of the joint capsule is suspected but not obvious, the traditional approach was to inject methylene blue into the joint to see if it emerged from the laceration. Normal saline is now preferred over methylene blue, as the latter can interfere with arthroscopy and cause an inflammatory reaction. The technique is simple. With sterile technique, sterile saline is injected into the knee joint at a location distant from the laceration. If saline emerges from the laceration, an open joint is diagnosed. Historically, 50 mL was the recommended volume, but nearly 200 mL is needed to achieve a sensitivity of 95%.20 This can be accomplished with intravenous fluid and tubing; maintenance of sterility is crucial. Anatomy and Pathophysiology: Knee dislocation refers to tibiofemoral dislocation and should not be confused with patellofemoral dislocation, a relatively minor injury. Knee dislocation is a limb-threatening emergency, because popliteal artery injury occurs frequently. Knee dislocation is uncommon but should be considered in the setting of an appropriate injury mechanism, because one half of all knee dislocations are reduced before the patient arrives at the ED.21 Reduction before ED arrival does not lessen the likelihood of vascular injury, and vascular injury should be considered in patients with severe ligamentous injuries and high-energy mechanisms. Knee dislocations are always associated with significant ligamentous injury. The joint capsule is disrupted, with accompanying trauma to the muscles and tendons. Injury to the popliteal artery is the most severe complication and is the primary cause of morbidity and limb loss.22,23 Anatomically, dislocations are described according to the displacement of the tibia relative to the femur. They are classified into five types: anterior, posterior, medial, lateral, and rotary. More than half of all dislocations are anterior and result from hyperextension. Posterior dislocations are the second most common type and usually result from high-velocity direct trauma to the flexed knee, often in association with vehicular trauma (dashboard impact).22 Clinical Features: The diagnosis of knee dislocation is based on the mechanism of injury and clinical and radiographic findings. When a dislocation is present, it is usually obvious. There may be no effusion after reduction, because the ruptured capsule allows blood and joint fluid to escape into the thigh and leg. Some experts have advocated expanding the definition of knee dislocation to include bicruciate ligament (i.e., ACL and PCL) injuries, even when the knee is reduced on initial presentation.21 For this reason, patients with grossly unstable knees but no proven dislocation and patients who have a bicruciate ligament injury should be evaluated for concomitant injuries, as with patients with known dislocation.4 Vascular injury is a catastrophic complication of knee dislocation, and popliteal artery injury is reported in 4.8 to 65% of these patients, depending on the mechanisms of injury in the population studied.4,22 The collateral geniculate arteries around the knee also may be damaged directly or secondarily compressed by hematoma formation after the dislocation. Direct arterial injury, decreased collateral circulation, and elevated compartment pressures all may compromise limb perfusion. In addition to being clinically occult, vascular injury in blunt trauma is more difficult to manage because of associated soft tissue injury and edema. “Hard” signs of vascular injury are absence of pulse, limb ischemia, rapidly expanding hematoma, pulsatile bleeding, and bruit or thrill over the wound, especially in penetrating injuries.24 Paresthesias in the leg should also lead to suspicion of injury to popliteal structures. When repair of a disrupted popliteal artery is delayed, the amputation rate increases with time, nearing 90% after 8 hours.23 The posterior tibial and dorsal pedal pulses should be evaluated but will be normal in 5 to 15% of popliteal artery injuries.25 Isolated intimal tears are usually managed without surgery, but a vascular surgeon should be consulted when such a tear is identified. Isolated intimal tears are not detectable on physical examination and are seen only angiographically or with duplex ultrasound. These injuries are treated with observation or anticoagulation alone but can result in popliteal artery occlusion during surgery. Injuries to small branches of the popliteal artery can be managed by observation and serial examinations, but vigilance for compartment syndrome is necessary.21 Neurologic integrity in the limb also should be assessed. Peroneal nerve injury is the most common major neurologic problem associated with knee dislocation; some degree of dysfunction occurs in 20 to 40% of patients and is permanent in approximately 80% of these.1,21,26 The peroneal nerve should be evaluated by determining sensation of the dorsum of the foot and by having the patient dorsiflex the ankle. Less commonly, the posterior tibial nerve may be injured, manifesting as diminished plantar sensation and plantar flexion of the foot. Complete nerve palsy in the acute setting is associated with a poor prognosis for recovery.26,27 Diagnostic Strategies: The diagnostic workup begins with an understanding of two crucial facts: half of all tibiofemoral dislocations are reduced before presentation, and injury to the popliteal artery is common with tibiofemoral dislocation regardless of whether there is spontaneous reduction or not. Therefore the diagnostic strategy is not applied only to the patient with known knee dislocation, but to any patient with a multiligament knee injury or with known or possible high-force trauma to the knee. The intubated multitrauma patient with ecchymosis around the knee may harbor an occult popliteal injury. The athlete with isolated knee trauma and no dislocation on presentation may end up an amputee.28 Serial physical examinations—meaning palpation of the pedal pulses—can detect most popliteal artery injuries, with a sensitivity of 79%, specificity of 91%, positive predictive value of 75%, and negative predictive value of 93%.24 This has led some authors to suggest physical examination alone as a screening tool. However, a miss rate of 7% is too high for such a devastating injury. Adding measurement of the ABI is thought to improve the sensitivity enough for safe clinical practice. The ABI is traditional in primary care and vascular surgery clinics, where it is used to monitor arterial narrowing caused by peripheral vascular disease. The index is simply the ratio of the systolic blood pressure measured in the standard humeral location to the systolic pressure measured at the ankle. An ABI of greater than 0.9 has been found to have a negative predictive value for popliteal artery injury of 100% in knee dislocation.24 Duplex ultrasonography is thought to be equivalent to angiography as a sensitive tool for detection of traumatic occlusion or disruption of the popliteal artery, though the sensitivity has not been quantified in the setting of knee dislocation.29 CT angiography is promising, but its sensitivity has not been quantified in this setting.17,30,31 The choice of diagnostic strategy depends on the patient’s presentation. At one extreme is the patient with obviously impaired leg perfusion. In this case, emergency angiography or surgical exploration are indicated. At the other extreme is the patient with knee trauma but no clear indication that a dislocation even occurred. Figure 57-4 depicts a safe and efficient algorithm.28 During the secondary survey, the dislocation is reduced, if present on presentation. The feet are examined, and if both are warm and well perfused, dorsalis pedis and posterior tibial pulses are palpable and symmetrical, and, in the awake patient, sensation is subjectively and objectively intact, the ABI is measured. If the ABI is above 0.9, the physical examination is repeated every 3 to 4 hours for 24 hours. If no abnormalities attributable to popliteal artery disruption are detected, no further emergent workup is indicated. Before surgery to repair associated injuries, the surgeon may choose to perform duplex ultrasonography to rule out an isolated intimal tear, which, though not important to detect in the ED setting, can lead to complications during surgery. If the pedal pulses are asymmetrical or the ABI is below 0.9, immediate angiography is indicated. If pedal pulses are absent, the foot is cool or otherwise appears poorly perfused, or there is an expansile popliteal hematoma, immediate surgical exploration is indicated, with or without an arteriogram. Management: The dislocated knee should be reduced immediately and before radiographic confirmation unless the diagnosis is in doubt. Neurovascular status should be documented before and after reduction. For patients being transferred from nontrauma centers to trauma centers, reduction should be attempted before transfer. Reduction usually can be accomplished with simple traction-countertraction, ideally with sedation. Lateral pressure may be required—for example, for an anterior dislocation, the femur can be pushed posteriorly while the tibia is pulled anteriorly—but care should be taken not to apply undue pressure to the popliteal fossa. Posterolateral dislocations may not be reducible because the medial femoral condyle and MCL secure the dislocated joint in place, in which case, emergent open reduction in the operating room is indicated.27 Because many reductions are unstable, the limb should be immobilized in a long leg posterior splint with the knee in 15 to 20 degrees of flexion, and popliteal artery injury sought, according to the algorithm shown in Figure 57-4. Loss and disability are minimized by expedient revascularization and primary arterial repair, heparinization when not contraindicated, repair of popliteal venous injury, and aggressive wound débridement. Open joints require prophylactic antibiotics. If the neurovascular structures remain intact after dislocation, the knee joint is reduced and allowed to rest for 2 to 3 days before reconstruction of the torn ligaments is considered.27,32 Delayed complications associated with traumatic knee dislocations include deep vein thrombosis, compartment syndrome, pseudoaneurysm, and arterial thrombosis. Compartment syndromes generally develop within 24 to 48 hours of the initial injury. Pseudoaneurysms are rare but may form several hours to months after popliteal artery injury.32 Heterotopic ossification is a poorly understood syndrome of calcification of the soft tissues of the knee.33 It has been observed in uninjured knees of patients who have sustained major trauma. In its most severe form, heterotopic ossification can cause dramatic decrease in knee mobility. Almost one half of dislocated knees are found to have subsequent heterotopic ossification, although the most function-limiting form may be limited to patients with a history of severe trauma.33 Anatomy and Pathophysiology: Distal femur fractures are uncommon, constituting approximately 4% of femur fractures.32 A high-energy mechanism of injury is required. An isolated fracture of the femoral condyle may occur, or the fracture may extend in a T or Y pattern to include the intercondylar or supracondylar region of the femur. Condylar fractures are intra-articular and may result in disruption of the articular surface with subsequent arthritis. Clinical Features: Patients with condylar or intercondylar fractures have pain and swelling in the distal femur and suprapatellar region and often are unable to bear weight. Examination may reveal shortening, rotation, and angulation of the extremity and tenderness to palpation along the medial or lateral joint line. Acute hemarthrosis is common and may be caused by intra-articular extension of the fracture or associated ligamentous injury. Distal neurovascular status should be documented. Any laceration in the region of the fracture represents an open fracture until proven otherwise. Diagnostic Strategies: Routine AP and lateral views should be obtained and usually show the fracture pattern and any significant displacement of fragments. In high-energy injuries, radiographs of the ipsilateral hip and tibia are required to exclude associated fractures. Occasionally, CT or MRI may be required to diagnose a nondisplaced fracture. MRI is more sensitive, although CT is more readily available. If signs of vascular impairment are present, consultation for angiography or surgical exploration should be obtained emergently. Management: After the initial examination, the leg should be splinted to prevent excessive motion of the fracture site. Early orthopedic consultation is advised. In a stable patient with an uncomplicated fracture, reduction may be done with skeletal traction, followed by immobilization. Intra-articular fractures generally are treated with open reduction and internal fixation. Distal femur fractures may be associated with thrombophlebitis, fat embolus syndrome, delayed union or malunion if reduction is incomplete or not maintained, intra-articular or quadriceps adhesions if the fracture is intra-articular, angulation deformities, and osteoarthritis, particularly affecting the patellofemoral articulation. Anatomy and Pathophysiology: The proximal end of the tibia is expanded into the medial and lateral condyles, the former having the greater surface of the two. Together they make up approximately three quarters of the proximal tibial surface, and their integrity is important for normal knee alignment, stability, and motion. The plateau normally slopes 10 degrees from anterior to posterior; on a straight AP view, the anterior and posterior portions of the plateau may not appear to be at the same level. In addition, the lateral plateau is slightly convex upward, whereas the medial is slightly concave upward. Tibial plateau fractures encompass many differing degrees of articular depression and displacement. Because the initial injury mechanism usually is a valgus stress with an abduction force on the leg, 55 to 70% of condylar fractures involve the lateral plateau. Medial plateau fractures typically result from adduction forces on the distal leg and account for 10 to 23% of these fractures; both plateaus are involved in 11 to 31% of cases.32 If the knee is extended at the time of injury, the fracture tends to be anterior. Posterior condylar fractures usually occur when the knee is flexed at the time of impact. The Segond fracture represents a bone avulsion of the lateral tibial plateau (Fig. 57-5). The avulsion occurs at the site of attachment of the lateral capsular ligament. On radiographs, an oval-shaped fragment can be seen adjacent to the lateral tibial plateau, which can be confused with an avulsion from the adjacent fibular styloid. Segond fractures are usually accompanied by ACL disruption and anterolateral rotatory instability. Most Segond fractures are caused by sports injuries, and the mechanism is almost always knee flexion with excessive internal rotation and varus stress. Clinical Features: Knee fractures cause pain, tenderness, ecchymosis, soft tissue swelling, and hemarthrosis when intra-articular. A valgus or varus limb deformity may be present and usually indicates a depressed fracture or concomitant leg fracture. The most important aspect of the initial examination is assessment of neurovascular status. Many tibial plateau fractures cause vascular complications. The popliteal artery is immobile in this region and branches into the anterior and posterior tibial arteries at the upper edge of the interosseous membrane. The popliteal artery may be injured by fragments from bicondylar or comminuted fractures involving the subcondylar area. Vascular impairment may result in distal circulatory compromise. Displaced fractures of the lateral condyle may produce peroneal nerve paralysis in addition to injury to the anterior tibial artery. Stretch of the peroneal nerve is the usual cause of injury. Soft tissue injuries also may involve the capsuloligamentous structures of the knee. Ligamentous injuries accompany tibial plateau fractures in up to 66% of cases, most often involving the ACL and MCL.34 Cruciate ligament injuries associated with tibial plateau fractures are associated with an increased incidence of late traumatic arthritis and a poor prognosis. Regardless of the type of treatment, operative or nonoperative, tibial plateau fractures with significant residual laxity fare poorly in comparison with stable fractures.35 Fractures of the tibial plateau generally carry a good prognosis, with good to excellent results reported in 90% of patients more than 20 years after injury; however, high-energy tibial plateau fractures generally are associated with a more guarded prognosis.36 In high-energy fractures, a large degree of articular depression, multiple displaced condylar fracture lines, and diaphyseal-metaphyseal extension and comminution in association with open injuries or an extensive internal degloving injury are poor prognostic signs.37
Knee and Lower Leg
Knee
Principles of Disease: Anatomy and Pathophysiology
Clinical Features
Physical Examination
Tests for Specific Injuries and Disturbances
Diagnostic Strategies
Angiography
Magnetic Resonance Imaging
Arthroscopy
Joint Injection
Knee Injuries
Distal Femur Fractures
Tibial Plateau Fractures
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Knee and Lower Leg



Only gold members can continue reading. Log In or Register to continue




