Fig. 43.1
Facet strain causing back pain after compression fracture
Persistent post-procedure pain prompts an x-ray or CT evaluation of the injected site, especially if the pain has changed or gets worse with movement or in a certain position. Fracture of the pedicle and ribs has been reported with kyphoplasty.
A new compression fracture is a common occurrence after kyphoplasty (Fig. 43.2). The bone cement (polymethyl methacrylate) does not have the same resilience as natural cancellous bone, probably contributing to an adjacent level vertebral compression fracture [15]. The evidence for this phenomenon is suggestive but not conclusive. Patients with preexisting vertebral compression fracture are at much higher risk for another fracture. A new fracture produces back pain or worsening of preexisting back pain. There may not be an inciting event for a new fracture. A physical examination may or may not reveal a focal tender point over the fractured vertebra. An MRI is still the best imaging modality to evaluate the spinal anatomy as well as to time the fracture. Leaking of bone cement outside the body of the vertebra also is common.
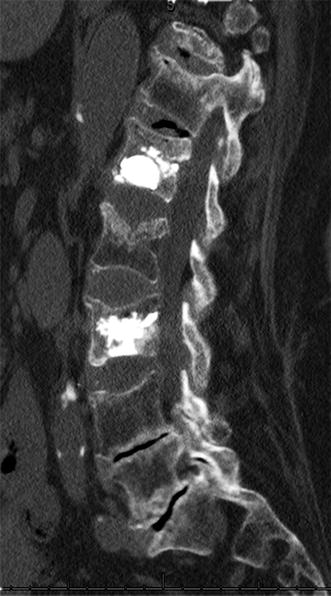
Fig. 43.2
Adjacent level fracture causing new or return of pain
The incidence is as high as 70%, depending upon the definition of leak and imaging modality used. Clinically not all leaks are equally significant. A leakage into the spinal canal resulting in cord compression can be devastating, requiring emergent decompressive surgery. Cement leak into a neural foramen can cause nerve root irritation or compression. The symptom is radicular pain after the procedure. If there is no sign of nerve root compression, i.e., motor weakness or loss of deep tendon reflexes, a leak is treated conservatively with an oral steroid or epidural steroid injection. Cement leak into the disc may accelerate degeneration of the disc or elicits an inflammatory response within the disc, leading to persistent back pain. A cement leak is prevented by injecting bone cement slowly and limiting the volume of injection.
Back pain also can arise from soft tissue damage or hematoma. Minimizing cannula manipulation will prevent these problems. In the absence of coagulopathy, hematoma formation is unlikely. Holding pressure at the injection site minimizes hematoma formation. Infection is rare but a reported complication. Infection may result in discitis, osteomyelitis, or epidural abscess. Common risk factors are a preexisting infection, diabetes mellitus, and immunosuppression. Staphylococcus aureus is often the isolated organism. Symptoms are worsening back pain and fever usually within a week to a month after the procedure. Inflammatory markers like C-reactive protein, erythrocyte sedimentation rate, and white cell count are elevated. MRI in the context of proper clinical picture confirms the diagnosis, but in some cases, a biopsy may be needed. Treatment is often surgery along with prolonged antibiotic therapy as many patients failed to improve with antibiotic alone. Cement laced with antibiotic as well as the periprocedure use of antibiotic has been suggested in immunocompromised patients. Patients with preexisting infections should be cleared of infection before getting kyphoplasty.
Vertebral augmentation therapy is a benign but not risk-free procedure. It relieves pain in selected patients [16]. Persistent pain after kyphoplasty requires systematic evaluation. If the pain is in the back and focal, then a physical examination rules out hematoma or bruising. A neurological deficit should be ruled out. If the pain is radicular or a neurological deficit cannot be ruled out, a prompt CT of the spine is obtained to rule out cement leak into the spinal canal or neural foramen or a rib or pedicle fracture (Fig. 43.3). Pain beginning days to weeks after a procedure may represent a new fracture or infection.
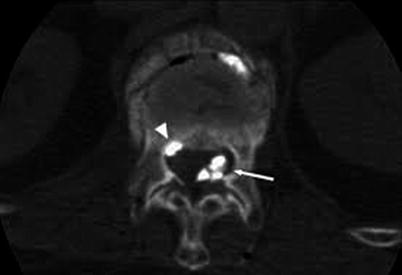
Fig. 43.3
Cement leakage into the foraminal space/epidural space
43.2.1 Algorithm for Persistent Back Pain
- 1.
Get Clinical Tree app for offline access
Immediate onset with no radiation
- (a)
Localized/non-radiatingRelated posts:
 A Case of Serotonin Syndrome in a Patient Receiving Epidural Steroid Injection for Chronic Low Back Pain
Pneumothorax After Paravertebral Block and Radiofrequency
Pneumothorax After Serratus Anterior Trigger Point Injection
A Case of Serotonin Syndrome in a Patient Receiving Epidural Steroid Injection for Chronic Low Back Pain
Pneumothorax After Paravertebral Block and Radiofrequency
Pneumothorax After Serratus Anterior Trigger Point Injection
 Sheared or Break of Caudal Catheters After Epidural Steroid Injection
Sheared or Break of Caudal Catheters After Epidural Steroid Injection
 Complications of Occipital Nerve Block
Complications of Occipital Nerve Block
 Intrathecal Ziconotide: Complications and Clinical Considerations
Intrathecal Ziconotide: Complications and Clinical Considerations

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



- (a)