88 Forearm Fractures
 Key Points
Key Points• The goal of treatment of forearm fractures is to restore length, correct angulation, and ideally, achieve normal function.
• Radiographs of the proximal and distal joints of patients with a forearm fracture should always be considered to rule out concurrent dislocations (i.e., Monteggia fracture).
Epidemiology
Injury is a leading cause of mortality, morbidity, and lost days of work. The annual health care cost of injuries exceeds $9.2 billion. Traumatic injuries result in more than 34 million emergency department (ED) visits each year.1 The highest rate of injuries occurs in persons between the ages of 15 and 24 years. Likewise, forearm fractures are commonly seen in young adults but have a bimodal distribution, with a second increased incidence in the elderly.2
Pathophysiology
The bones of the forearm consist of the radius and ulna. These two bones lie in parallel and are connected by joint capsules at the elbow and at the wrist, whereas the shafts are interlocked by a fibrous interosseus membrane.3 Most forearm fractures are caused by a sudden force, such as a fall on an outstretched arm. Because of the interlocking joint capsules, interosseus membrane, and contraction of the forearm muscles, multiple fractures, displaced fragments, and concurrent dislocations may be present. Alternatively, forearm fractures may be due to smaller repetitive injuries, which result in a stress fracture over time. Any pathophysiologic process that reduces the integrity of the bone, such as osteopenia, osteomyelitis, and bone metastasis, increases the likelihood of fracture, even with normal external stress.4
Presenting Signs and Symptoms
Symptoms of forearm fractures include pain, forearm edema, forearm ecchymosis, abnormal or reduced mobility from the wrist through the elbow, and complaints of neurovascular compromise. Findings on physical examination can include obvious bony deformity; shortening of the forearm; crepitus; tenderness to palpation of the forearm; joint effusions; abnormal mobility of the wrist, forearm, or elbow; and neurologic and vascular deficits of the forearm, wrist, or hand. Box 88.1 lists the signs and symptoms of fractures and complications that indicate serious injury.
Box 88.1 Signs and Symptoms of Fractures and Complications That Suggest Serious Injury
In general, forearm fractures are classified by the bone (or bones) involved, anatomic location, trajectory of the fracture and alignment of the fracture fragments, and the presence of angulation, rotation, comminution, and concurrent dislocations. All fractures should be further described as open or closed, and the presence (or absence) of distal neurologic and vascular function should be noted (Fig. 88.1).
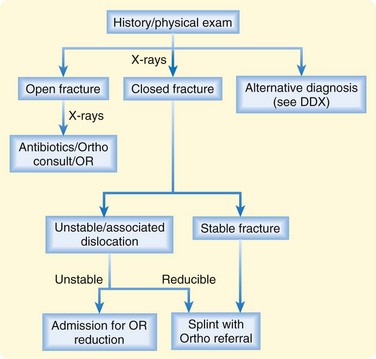
Fig. 88.1 Approach to patients with a suspected forearm fracture.
DDX, Differential diagnosis; OR, operating room; Ortho, orthopedics.
Types of forearm fractures that are frequently mentioned in the medical literature are described in Table 88.1.
Table 88.1 Types of Forearm Fractures
| NAME | DESCRIPTION |
|---|---|
| Colles | Distal radial extension fracture (may also include the ulna) with dorsal displacement of the distal fragments |
| Smith | Distal radial flexion fracture with volar displacement of the distal fragments |
| Barton | Intraarticular fracture of the dorsal rim of the distal end of the radius, often associated with carpal dislocation. Treatment is typically operative |
| Hutchinson | Radial styloid fracture associated with carpal dislocation |
| Galeazzi | Distal radial shaft fracture with concurrent distal radioulnar dislocation |
| Monteggia | Ulnar shaft fracture with dislocation of the radial head |
Pediatric Fractures
Forearm fractures in the pediatric population include several additional entities because children have a plastic bone matrix and active growth plates, both of which contribute to unique fractures (Table 88.2). In children, when an external force bends a long bone, one side of the cortex may be disrupted while the other side remains intact (greenstick fracture). Alternatively, a deformity of the bone may occur without an obvious fracture line (plastic deformity). With compression, buckling of the cortex may be seen (torus fracture). Depending on the age of the child, fractures through the various growth plates of the elbow and wrist may also occur (Salter-Harris fractures).5
Table 88.2 Types of Pediatric Fractures
| NAME | DESCRIPTION |
|---|---|
| Torus | Fracture involving compression buckling of one or both sides of the cortex |
| Greenstick | Fracture involving distraction of one side of the cortex without apparent disruption of the other |
| Plastic deformity | Bowing of the radius or ulna without obvious fracture lines (multiple microfractures) |
| Salter-Harris | Fracture involving the growth plates |
Differential Diagnosis and Medical Decision Making
The differential diagnosis for forearm fractures includes any soft tissue injury to the forearm, in addition to acute skin, soft tissue, and joint infections (Box 88.2). Some clinical aspects of acute arterial occlusion, as well as venous thrombosis, may mimic forearm fractures. Any acute neurologic change, including paresthesias, weakness, and functional loss, should be considered along with forearm fractures. Two normal variants sometimes mistaken for forearm fractures on radiographs are normal growth plates in children and nutrient vessels.







