159 Fluid Management
 Key Points
Key Points• Shock is defined by inadequate tissue perfusion and not by systemic blood pressure.
• The majority of emergency department patients who require resuscitation are in compensated shock with normal blood pressure.
• Volume expansion with isotonic fluid is the most important immediate therapy for most patients with circulatory insufficiency.
• Resuscitation and maintenance fluids should be tailored to an individual patient’s acid-base and electrolyte status.
• The fluid dose titrated to appropriate end points is more important than the individual fluid class (i.e., crystalloid versus colloid) used for resuscitation.
• Normal vital signs do not guarantee adequate systemic perfusion and should not be the ultimate end point of resuscitation.
• Dynamic measures of fluid responsiveness should be used to assist in the management of patients who remain hypoperfused despite initial empiric volume therapy.
Perspective
Hypovolemia is a common crisis in acute care medicine. Loss of volume is often a direct consequence of acute fluid or blood loss, but relative hypovolemia complicates many clinical conditions. Its severity ranges from mild compensated hypovolemia to shock and hypotension that place end-organ perfusion and function at risk. Fluid therapy to optimize cardiac performance and restore fluid and electrolyte balance is a cornerstone of medical support. Timely and appropriate fluid therapy maintains macrocirculatory and microcirculatory support and reduces mortality.1 In contrast, both underresuscitation and overly aggressive fluid therapy can have an adverse impact on organ function and outcome.2,3 Inadequate resuscitation risks leaving a patient in compensated shock. Overly aggressive fluid administration results in volume overload without improving oxygen delivery and is associated with worse clinical outcomes.4 In addition to sustaining circulating blood volume, intravenous (IV) fluids also correct and maintain normal acid-base and electrolyte balance. A thorough understanding of the appropriate selection, timing, and goals of fluid therapy is vital to optimize patient care.
Pathophysiology
Water
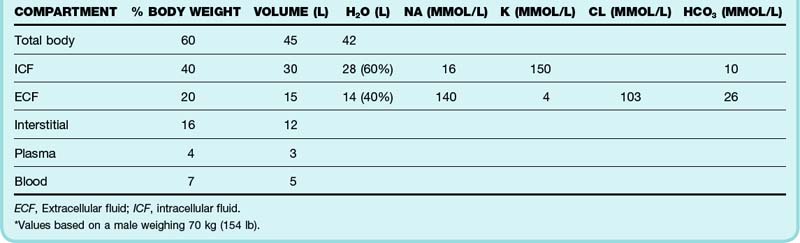
Water is the most abundant constituent of the body. An adult man weighing 70 kg (154 lb) contains approximately 45 L of water, which accounts for 60% of body mass (Table 159.1). Total body water (TBW) is proportional to lean body mass and affects maintenance fluid requirements. TBW is physiologically compartmentalized into intracellular and extracellular spaces. The extracellular compartment is anatomically and conceptually divided into vascular and interstitial spaces.
Presenting Signs and Symptoms
Absolute hypovolemia occurs as a consequence of loss of water, electrolytes, or blood (or any combination of the three) (Box 159.1). Patients with hypovolemia most often have symptoms related to reduced cardiac output such as fatigue, dyspnea, postural dizziness, and near or true syncope. Tolerance is variable and depends on the acuity and severity of the hypovolemia, associated anemia, individual physiologic reserve, and primary cause. Organ dysfunction is often a heralding sign of hypovolemia and may occur in the absence of global hypoperfusion or frank hemodynamic instability.
Shock is defined as a state of inadequate tissue perfusion in which oxygen delivery does not meet metabolic requirements. The term does not reflect perfusion pressure—shock may occur with low, normal, or elevated blood pressure. Unfortunately, clinical signs are unreliable indicators of oxygen delivery and blood volume.5,6
Compensated shock refers to inadequate perfusion in the setting of normal blood pressure. The majority of critically ill patients are in compensated shock. The difficulty in identifying these patients prompted the terms occult and cryptic shock to describe normotensive patients with alternative evidence of cardiovascular insufficiency. Hyperlactatemia (<3 mmol/L) is an important marker to aid in identification of these high-risk patients.7 Left unresuscitated, these patients often progress to frank hypotension.
Brief episodes of hypotension are important markers of hypoperfusion and herald progressive hemodynamic deterioration. These self-limited episodes of transient hypotension represent progressive exhaustion of cardiovascular compensation and are the first sign of uncompensated shock.8 Uncompensated shock is characterized by hypotension that occurs when physiologic attempts to maintain normal perfusion pressure are overwhelmed or exhausted. Sustained hypotension signifies a late stage of shock.
Volume status and perfusion should be evaluated during every emergency department (ED) examination (Box 159.2). Delayed capillary refill, dry axillae and mucous membranes, abnormal skin turgor, sunken eyes, and a depressed fontanelle are classic but imperfect hallmarks of hypovolemia.9,10 Peripheral cyanosis, cool extremities, and cutaneous mottling (cutis marmorata) characterize classic hypodynamic shock but are not a primary indication of hypovolemia. In contrast, early hyperdynamic septic shock may be manifested as peripheral vasodilation with warm extremities and brisk capillary refill.
 Priority Actions
Priority Actions






