120 First Trimester Ultrasonography
 Key Points
Key Points• Patients with ectopic pregnancy have highly variable and often unhelpful findings on physical examination.
• Ultrasound is the initial imaging modality of choice to locate a pregnancy in the first trimester.
• Emergency physicians proficient in ultrasound are capable of rapidly diagnosing ectopic pregnancy and expediting definitive care.
• Most first trimester pregnancies can be localized within the uterus on initial ultrasound in the emergency department.
• All patients discharged from the emergency department without a confirmed intrauterine pregnancy by ultrasound should thoroughly understand the “ectopic precautions,” have close outpatient follow-up arranged with their obstetrician, and have the means to return immediately to the emergency department if complications arise.
Introduction
All female patients of reproductive age seen in the emergency department (ED) with vaginal bleeding or abdominal or back pain should have a urine or serum pregnancy test performed. Ectopic pregnancy is the number one cause of death in patients in the first trimester.1 Emergency physicians (EPs) caring for these patients understand that no historical clues or physical findings can effectively affirm or refute an ectopic pregnancy.2 The rate-limiting step is finding the location of the pregnancy. Ultrasound imaging and interpretation play a crucial role in this decision-making process. The faster this information is available, the quicker management can be implemented. In the late 1980s, a few EP pioneers invested the time and effort to learn the technical and interpretive skills necessary to bring ultrasound to the bedside.3 The ability to locate a first trimester pregnancy saves valuable time in the search for an ectopic pregnancy.4 Ultrasound performed at the patient’s bedside quickly classifies patients by ultrasound criteria.5 Based on this ultrasound classification, management strategies can be implemented. The following sections describe the ultrasound techniques and management skills used in symptomatic patients in the first trimester of pregnancy.
Evidence-Based Review
In most EDs, when “formal” ultrasound is traditionally ordered, it is actually performed in the department of radiology. This requires (1) time to transport the patient out of the ED, (2) a sonographer available to obtain the images, and (3) a radiologist to interpret the study. Ultimately, the combination of these factors postpones the diagnosis, delays definitive care, and increase the patient’s length of stay.4 As an alternative to formal ultrasound, many EPs have learned how to perform and interpret ultrasound images at the patient’s bedside. As early as 1989, a number of small studies suggested that EPs were able to perform ultrasound for ectopic pregnancies with high sensitivity.3 When previous studies from multiple institutions are compiled to increase the sample size (N = 2057), it is estimated that EPs have a pooled sensitivity of 99.3% when diagnosing ectopic pregnancies at the bedside. Sensitivity is defined as the proportion of bedside ultrasound images demonstrating a true absence of definitive intrauterine pregnancy (IUP) in patients with ectopic pregnancies.4
Multiple retrospective and prospective studies from the late 1990s and early 2000s have reported that when compared with formal imaging, the use of bedside ultrasound to evaluate first trimester bleeding reduced length of stay in the ED by a mean time of 48 to 169 minutes. Time of day, day of the week, and whether ultrasound technicians were in house 24 hours a day were some of the factors that had an impact on the length of stay.5 Finally, based on two separate studies from the early 2000s, bedside ultrasound performed by EPs saved an estimated $229 to $1244 per ED visit when compared with patients who underwent radiology-performed ultrasound. In some cases this was a 40% savings in billed charges.5 Literature from the past 20 years has and continues to demonstrate that ultrasound performed by an EP to evaluate for ectopic pregnancies is feasible, fast, and accurate. Bedside ultrasound in symptomatic first trimester pregnant patients has high sensitivity in ruling out ectopic pregnancy, speeds time to diagnosis, and decreases true costs.
How to Scan
Transabdominal Technique
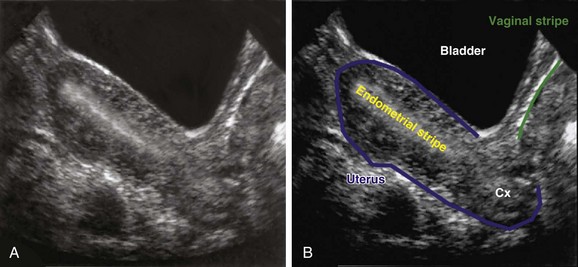
In the sagittal view, in which the uterus is seen in its long axis, the probe is placed just superior to the pubic symphysis with the indicator pointed toward the patient’s head. The anterior-most organ on screen is the fluid-filled, triangular-shaped bladder. Just posterior to the bladder is the pear-shaped uterus. The uterus more commonly lies in an anteverted position, with the fundus pointed toward the anterior abdominal wall, but it may also be seen in a retroverted lie with the fundus pointing posteriorly toward the spine. The endometrial stripe serves as the landmark for identifying the longitudinal uterus in the midline. The endometrial stripe is a result of the endometrial mucosal lining coming together to form a hyperechoic, curvilinear line that continues as the cervical stripe more inferiorly (Fig. 120.1, A and B). After the midline of the longitudinal uterus is identified, the probe is panned from side to side to evaluate the entire width of the uterus. Much of the hyperechoic area surrounding the uterus is the bowel and rectum, which are poorly defined because of their solid and gas contents.
Endovaginal Technique
The arrival of endovaginal transducers in the 1980s significantly improved the quality of ultrasound imaging in female patients. Simplified, the engineering design placed an ultrasound transducer on the end of a stick that could be inserted into the vaginal vault. This permits the transducer scanning head to be in close proximity to the pelvic organs, which has several important implications in ultrasound imaging. First, there is a clearer path to transmit and receive echoes, and second, the shorter distance between the transducer and the pelvic organs allows higher transducer frequencies to be used.6 In contrast to the transabdominal approach, the quality of images from an endovaginal approach is enhanced with an empty bladder because of less distortion of the pelvic anatomy.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


