(1)
Chennai Breast Centre, Chennai, India
The terminal ductal lobular unit is normally 1–2 mm in size but can vary from 1 to 8 mm in size. Around the time of menopause, the production of new TDLUs decrease along with the atrophy of lobules and connective tissue surrounding the TDLUs. They are partially replaced by adipose tissue. Mammographically this is well demonstrated as fatty breasts in the postmenopausal age group.
Fibrocystic change (cystic hyperplasia) includes various forms of adenosis and epitheliosis, cyst formation, fibrosis, and apocrine metaplasia. The term fibrocystic disease should be avoided as fibrocystic changes are considered to be a range of normal variation in the process of involution (Fig. 17.1).
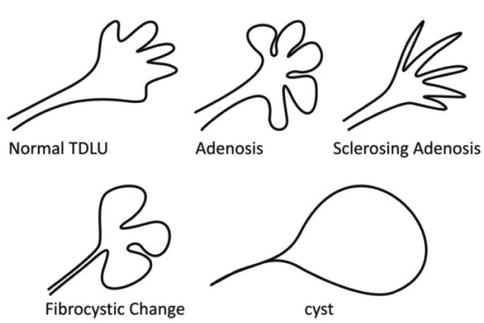
Fig. 17.1
Schematics representing the normal terminal ductal lobular unit which measures 1–2 mm in size, adenosis which is enlargement and multiplication of TDLU’s, distorted TDLU’s in sclerosing adenosis and involuting ducts results in micro- and macrocysts
Adenosis
Adenosis is multiplication of acini in a disorderly manner. The lobular pattern is maintained.
Fibrosis
Fibrosis develops at a later stage of adenosis. This is represented in the mammograms as dense breast with a ground glass appearance that is featureless. The extensive fibrosis masks the parenchymal changes, thereby making cancer detection difficult in dense breasts.
Ductal Hyperplasia
Ductal distension and cellular proliferation are the characteristic features of hyperplasia. Microscopic evaluation of the cells and their nuclei and proliferative patterns is required to distinguish usual type hyperplasia, atypical hyperplasia, and DCIS. Patients may give a history of cyclical mastalgia and nodularity. Persistent dominant nodules that are palpable clinically require further evaluation.
Mammographic Findings
Ductal hyperplasia is often an incidental finding in breast biopsies done for clinical or mammographic findings. The secretions associated with usual type hyperplasia and florid atypical ductal hyperplasia calcifies. These calcifications tend to be diffuse, scattered, and bilateral. Morphologically they are mostly round, punctuate, or amorphous. Apart from standard CC and MLO views, lateral views (90″ projection) and magnifications will be required to study the morphology in detail. Majority of these calcifications can be dismissed as benign. Indeterminate calcifications need biopsy to rule out a malignancy.
Ultrasound Findings
Ultrasound findings vary from very echogenic breast tissue due to fibrosis to complex solid and cystic masses. Some of them can even be irregular with shadowing, often requiring a biopsy. There may be scattered echogenic foci due to calcifications.
Histological Features
Usual Type Hyperplasia
The term refers to intraluminal epithelial proliferation without atypia, involving the terminal duct lobular units or interlobular ducts. The proliferation is categorized as mild if the epithelium is 3–4 layers thick, moderate if more than four cell layer thick, and florid if there is a marked enlargement of the affected ducts.
The key features are:
A heterogeneous population comprising epithelial cells, myoepithelial cells, and apocrine cells
A syncytial growth pattern due to indistinct cell margins
Irregular and slit-like, peripherally situated lumina
Oval nuclei oriented parallel to the long axis of the cells (streaming)
Tapering cell bridgesRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree







