(1)
Chennai Breast Centre, Chennai, India
Fibroadenomas are benign tumors that commonly occur in the early reproductive age group. They are hyperplastic, benign fibroepithelial lesions of the breast composed of both stromal and epithelial components. They arise from the terminal ductal and lobular units. Since they originate from the terminal ductal lobular units with the surrounding stroma, they can have the entire spectrum of benign proliferative changes. Fibroadenomas exhibiting these benign proliferative changes are classified as complex fibroadenomas.
The etiology of fibroadenomas is unclear, but estrogen is thought be the stimulus. It is common in young women and the risk decreases with increasing age. Epstein–Barr virus is associated with rapidly growing fibroadenomas in immunocompromised patients, but their role in nonimmunocompromised patients is not clear.
Fibroadenomas are firm, rubbery, elliptical, or gently lobulated in shape. They are freely mobile and often described as a breast mouse. They are encapsulated by a thin rim of compressed breast tissue. Histologically they are of two types – intracanalicular and pericanalicular. Pericanalicular fibroadenomas have stromal tissue surrounding the ducts, and the intracanalicular fibroadenomas have the ducts compressed into slits by the stroma (Fig. 19.1). They are indistinguishable on mammography or ultrasound and purely a histological classification with no differences in the natural history or the outcome. Some fibroadenomas contain both intra- and pericanalicular elements. Sometimes the intracanalicular fibroadenomas are difficult to distinguish from a phyllodes tumor, particularly on a core biopsy.
Fig. 19.1
Low-power view of fibroadenoma: proliferated ducts in a hypocellular stroma. High-power view of fibroadenoma showing compressed ducts in a uniform stroma
Fibroadenomas are usually solitary, but about 15–20 % of them are multiple, more so in the Asian and Afro-Caribbean population. Occasionally they can grow rapidly and enlarge even to 10 cm or more. These are called giant fibroadenomas or juvenile fibroadenomas. About 30 % of them involute and disappear spontaneously. Some of them can undergo infarction, necrosis, and calcification. Infarcted fibroadenomas tend to become irregular in shape and become adherent to the surrounding tissue with appearances that are suspicious for malignancy.
Risk of Malignancy
Since the fibroadenomas arise from TDLUs with ductal and stromal components, they behave just like normal breast tissue and can develop a ductal or lobular carcinoma in situ and invasive malignancy. The incidence of malignancy in a fibroadenoma is 1 in 1,000. The complex fibroadenomas and associated family history of breast cancer increase the relative risk of breast cancer to 2.17 times than normal.
Mammography Features
The typical fibroadenoma on a mammogram appears as a circumscribed, oval, isodense mass lesion with smooth margins. In very young women with dense breasts, the normal dense breast tissue may obscure the mass lesion entirely or partially with indistinct margins.
Not all fibroadenomas have smooth margins or appear isodense. Hyalinized fibroadenomas may appear more dense than surrounding breast tissue. Infarcted fibroadenomas may have irregular and angular margins.
With increasing age the fibroadenomas can degenerate and can have dense coarse macrocalcifications which resemble a popcorn. Some may just have rim-like calcifications in the periphery of the lesion. At some point, before the calcification develops into a classical popcorn-like involuting fibroadenoma, they appear very irregular and pleomorphic making it difficult to distinguish it from a malignancy (Figs. 19.2a–d and 19.3a–d).
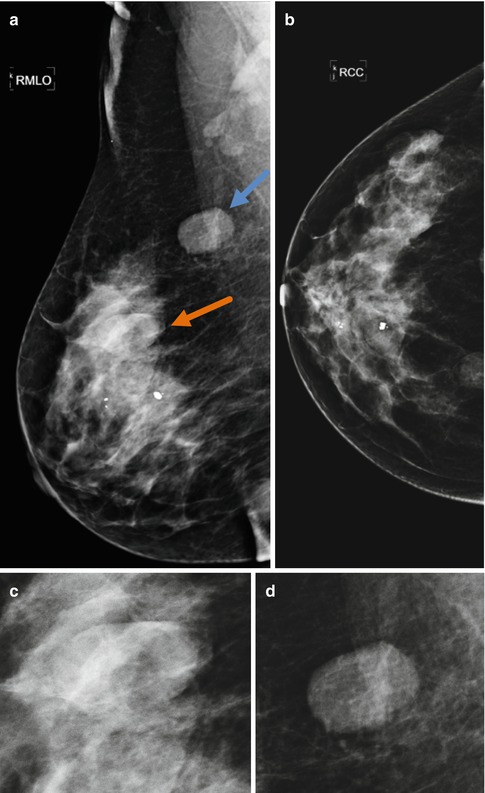

Fig. 19.2
(a, b) Right breast CC and MLO views show a well-circumscribed ovoid isodense opacity in the upper quadrant seen better in MLO view. Another isodense ovoid opacity is seen in the upper quadrant with partial halo and partly obscured by surrounding dense parenchyma. Arrows point to the lesion. (c, d) Magnified images showing the fibroadenoma
Fig. 19.3
(a–d) Images showing calcifications in various stages in fibroadenomas undergoing hyalinization. (a) Magnified mammogram image showing an isodense opacity with irregular margins and associated pleomorphic calcifications. (b) Magnified mammogram image showing a low density ovoid opacity with coarse “popcorn“ calcifications. (c) Magnified mammogram image showing dense ovoid opacity with surrounding halo and associated heterogeneous calcifications. (d) Magnified mammogram image showing a low density mass with coarse heterogeneous calcifications
Ultrasound Features
Classical fibroadenomas show the following features:
Mass shape – described as oval or elliptical or transversely oriented.
Mass margins – circumscribed or gently lobulated (less than 3 lobulations).
Echogenicity – isoechoic or mildly hypoechoic to fat.
Acoustic transmission – normal or enhanced.
Orientation – wider than taller.
Thin echogenic capsule.
Edge shadows are usually seen.
Fibroadenomas are encapsulated by a rim of normal breast tissue. The presence of this pseudocapsule gives the appearance of a thin echogenic capsule all round (Fig. 19.4). This is a very important feature of benignity along with the other features. The thin pseudocapsule at the edges produces thin edge shadows which also are a feature of benignity (Fig. 19.5). Parallel growth pattern along the paths of least resistance in the tissue planes indicates that it is a benign lesion, i.e., wider than taller. As they enlarge in size, they are less likely to remain elliptically shaped, and they develop more lobulations. The presence of more than 3 lobulations or microlobulations would be classified as BI-RADS 4a, which mandates a biopsy (Fig. 19.6).