115 Emergency Renal Ultrasonography
 Key Points
Key Points• The presence of unilateral hydronephrosis in the correct clinical context is used as an indirect finding for the diagnosis of renal colic. Obstructing stones are not typically visualized directly during bedside sonography.
• Identification of hydronephrosis in one kidney should prompt evaluation of the contralateral side to rule out bilateral hydronephrosis as a result of bladder outlet obstruction.
• Ultrasound measurements of the urinary bladder can be used to estimate bladder volume and identify a distended bladder in patients with suspected urinary retention.
• Abdominal aortic aneurysm should always be included in the differential diagnosis of renal colic. Emergency practitioners should maintain a low threshold for performing screening ultrasound of the aorta in patients with risk factors for an aneurysm.
Evidence-Based Review
Computed tomography (CT) currently has the greatest sensitivity and specificity of imaging modalities used for the diagnosis of renal colic. When compared with ultrasound, non–contrast-enhanced CT is more sensitive in identifying obstructing ureteral stones1–4 and more accurate in measuring stone size.4,5 CT also more consistently locates the specific site of obstruction along the course of the ureter and can identify other causes of abdominal pain that may mimic acute renal colic.
However, routine use of CT for suspected renal colic has significant limitations. Patients are exposed to significant amounts of ionizing radiation when they undergo CT of the abdomen and pelvis,6,7 which makes CT inadvisable during pregnancy and less appealing in the pediatric population. Because renal colic is a recurrent diagnosis, patients may eventually receive multiple CT scans over time, and cumulative radiation doses may rise to concerning levels8 and place patients at risk for cancer later in life. Additionally, radiologic imaging has been shown to be the largest contributor to the cost of hospitalization in patients with renal colic, with CT being the most expensive imaging modality.9,10
Ultrasound offers a safe, noninvasive means of assessing for renal colic that does not subject the patient to any ionizing radiation. Traditionally, ultrasound has been thought to have only fair sensitivity (37% to 64%) for detecting stones and better sensitivity (74% to 85%) for the diagnosis of acute obstruction,1 whereas CT has consistently shown sensitivity greater than 90% for the diagnosis of ureteral stones.1–4 Recent studies using modern ultrasound equipment in the hands of skilled operators have demonstrated comparable sensitivity (76% to 98%) of ultrasound for the detection of ureteral stones.11–14 Although specific stone location and size cannot always be determined with ultrasound, surrogate findings may have prognostic value in guiding patient management. One study showed that normal renal ultrasound findings in the setting of suspected renal colic predicted a very low risk (0.6%) for subsequent urologic intervention.15
The goal of bedside ultrasound is to identify unilateral hydronephrosis as an indirect sign of obstructing ureteral stones. In the emergency department setting, Rosen et al. demonstrated a sensitivity of 72% and specificity of 73% for the detection of hydronephrosis with bedside ultrasound.16 More recently, Gaspari and Horst reported a sensitivity of 87% and specificity of 85% for the diagnosis of hydronephrosis.17 These results are comparable to a sensitivity of 81% and specificity of 92% for bedside ultrasound performed by on-call urologists; however, this study evaluated other renal findings in addition to hydronephrosis.18 Although the specific size of the obstructing stone is not typically demonstrated on bedside ultrasound, the degree of hydronephrosis may correlate with the size of the obstructing stone. A 2010 study showed that no or mild hydronephrosis predicted smaller stone size (<5 mm) as opposed to moderate or severe hydronephrosis.19
Bedside ultrasound for the measurement of urinary bladder volume has been well described in the literature. Bedside ultrasound provides a quantitative assessment of bladder volume when evaluating for urinary retention in the emergency department setting and can guide the need for emergency catheterization.20,21 Many studies have shown good correlation between sonographic bladder volume calculations and urine volumes obtained via catheterization.22–24 In the pediatric population, ultrasound has been shown to predict patients with volumes sufficient for successful catheterization of urine samples (>3 mL).25–28 This may help avoid multiple attempts at urinary catheterization, which can result in unnecessary patient discomfort and the potential for iatrogenic infection. Additionally, bedside ultrasound has demonstrated increased success rates during attempts at suprapubic aspiration when compared with traditional, landmark-based techniques.29–31
How to Scan
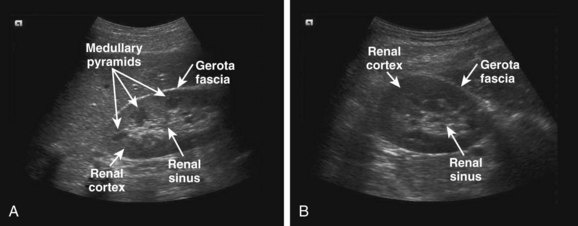
For the right kidney, the probe is initially placed along the lower portion of the rib cage in the midaxillary line with the probe marker directed toward the patient’s head. The resulting coronal view is the traditional right upper quadrant view of the focused assessment with sonography for trauma (FAST) examination. The kidney lies in a plane oblique to the long axis of the body, and the probe usually needs to be rotated slightly counterclockwise to obtain a maximally longitudinal view of the kidney (Fig. 115.1, A). This orientation also helps the ultrasound transducer align the image in between the ribs, thus minimizing rib shadows. The transducer should then be angled anterior to posterior so that it fans through the entire kidney. To obtain a transverse view of the kidney, the probe is rotated 90 degrees in a counterclockwise direction (Fig. 115.1, B). The transducer should then be fanned superior to inferior to image the entire kidney in the transverse plane.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


