Emergency Preparedness for and Disaster Management of Casualties from Natural Disasters and Chemical, Biologic, Radiologic, Nuclear, and High-Yield Explosive (Cbrne) Events
Preparing to manage, deal with the sequelae of, and mitigate future disasters originating from natural events, industrial accidents, or of more interest recently, caused intentionally by terrorists using chemical, biologic, radiologic, nuclear, or high-yield explosive (CBRNE) agents is a high priority for the majority of governments the world over (Murray MJ. Emergency preparedness for and disaster management of casualties from natural disasters and chemical, biologic, radiologic, nuclear, and high-yield explosive (CBRNE) events. In: Barash PG, Cullen BF, Stoelting RK, Cahalan MK, Ortega R, Stock MC, eds. Clinical Anesthesia. Philadelphia: Lippincott Williams & Wilkins; 2013:1535–1552) (Table 53-1). The American Society of Anesthesiologists has recognized the importance of such activities and in the past decade has established a Committee on Emergency Preparedness and Trauma and a Global Health Initiative. Certain principles are common to all such events independent of their etiology, and as a group, anesthesiologists are as well prepared if not better prepared to assist their communities in planning for and in caring for patients from a disaster.
I. Preparation: Personal Preparedness
Family Plan
Often overlooked during emergency preparedness and disaster management training is the development of a family plan and a personal preparedness plan.
Plans might include situations such as what to do if there is a fire, what to do if parents do not make it home, the location of second copies of all important documents,
and where to meet if the house or neighborhood is destroyed or not accessible.
Many assume that they will be able to communicate with loved ones during a disaster, but often cell phone towers are damaged or so many people are trying to use the system that they network is overwhelmed. Plan in advance so that you are prepared for these contingencies.
Government Plan (Fig. 53-1)
Nongovernment Organizations
Ever since the anthrax attacks of 2000 and 2001, the destruction of the World Trade Center Towers on September 11, 2001, the SARS epidemic of 2004, and the continued devastation caused by nature (hurricanes, earthquakes, tornadoes, floods, and fires), The Joint Commission (TJC), the American Hospital Association, and state and county health departments have more closely monitored and evaluated hospitals’ and communities’ emergency preparedness.
Despite the best effort of law enforcement, fire and rescue teams, and emergency medical agencies, hospitals will continue to play a vital role in helping communities respond to catastrophic events.
TJC has been proactive in recognizing the need for a “surge capacity” within health care systems to handle the large number of patients who might be victims of catastrophic events.
Table 53-1 Examples of Chemical, Biologic, Radiologic, Nuclear, and High-Yield Explosive Events | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
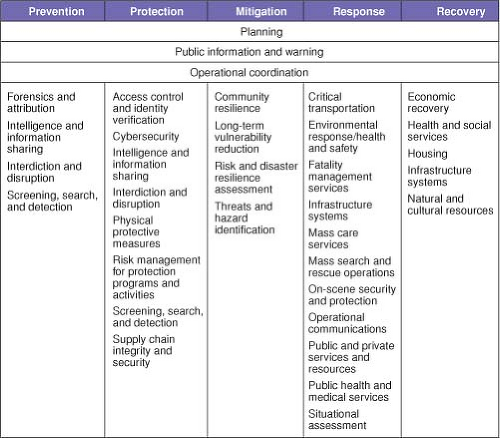 Figure 53-1. The multiple issues for which the Federal Emergency Management Agency must prepare and with which agencies it must coordinate—the US Departments of Justice, Health and Human Services, Agriculture, Commerce, and Defense. |
II. Role of Anesthesiologist in Management of Mass Casulties
Anesthesiologists basic understanding of physiology and pharmacology, and their airway skills, fluid resuscitation expertise, and ability to manage ventilators and to provide anesthesia in the field environment, in the emergency
department, in the operating room (OR), and in intensive care units (ICUs) will be invaluable.
During a mass casualty incident, an anesthesiologist may well be asked to provide anesthetic services in an area other than the OR or ICU.
Triage
If assigned to triage patients, the anesthesiologist will be expected to classify patients into four groups—those requiring immediate care, delayed care, first aid, and expectant (not expected to survive inadequate resources to adequately resuscitate without jeopardizing the lives of patients more likely to survive).
In the future, biotechnology may play a role, but at present, hospitals must rely on physicians’ experience
As emotionally difficult as the process might be of identifying or managing patients not expected to survive is the assessment of patients who may have been injured or been affected during a disaster but do not appear to require treatment but who might require delayed care (Table 53-2).
Decontamination
Decontamination is normally performed first and then patients are evaluated and triaged. (Clothes are removed, and individuals are washed with copious amounts of water, and if they have been exposed to a chemical agent a dilute solution of sodium hypochlorite, 0.5% [household bleach] can be used.)
If the patient presents with life-threatening injury (acute respiratory failure requiring emergency tracheal
intubation), the patient is treated first and decontaminated afterward.
The intubation must be performed with the anesthesiologist wearing a hazard materials (HAZMAT) or a biohazard suit with multiple-layered gloves and a gas mask.
Consider securing the airway with a laryngeal mask airway, when indicated, rather than with a tracheal tube.
Emergency Department
Depending on the types of casualties but especially for casualties from a violent explosion, anesthesiologists might be assigned to manage patient’s airways and secure central venous access.
Anesthesiologists should position themselves at the head of the bed and assume responsibility for the airway and venous access.
If chemical weapons are also used, not only may tracheal intubation be required, but ventilator management may also be necessary.
Table 53-2 Evaluation of Patients Who Do Not Require Immediate Treatment But May Require Delayed Care | |||
|---|---|---|---|
|









