215 Emergency Medical Services and Disaster Medicine
 Key Points
Key Points• Emergency medical services (EMS) consist of a heterogeneous group of entities that vary according to urbanization, training procedures, skill level of practitioners, resources, and scope.
• Although EMS research is developing rapidly, controversy exists over the role of EMS interventions and protocols in commonly encountered conditions such as trauma and cardiovascular emergencies.
• Disaster medicine encompasses planning, resource allocation, and health care response to any event—natural or man-made—that overwhelms the resources of a particular locality.
• Weapons of mass destruction have the potential to cause severe physical damage and health concerns that require specific, targeted planning and coordination for emergency care personnel.
Introduction and History
An emergency medical services (EMS) system can be defined as “a coordinated arrangement of resources (including personnel, equipment, and facilities) organized to respond to medical emergencies, regardless of the cause.”1 Modern EMS systems in the United States have their origins largely in battlefield medicine.2–6 Indeed, it was a surgeon in the Napoleonic military campaign who pioneered the concept of rapid response to injured soldiers in the field of combat.3 Baron Larrey, the “father of modern prehospital care,” developed a systematic approach to combat trauma in which ambulances transported wounded soldiers from the battlefield to organized medical stations. In the American Civil War, ambulances were placed under structured medical direction. Successive advances in technology and EMS organization in later wars resulted in significantly decreased mortality rates for battle combatants who were transported to field hospitals.5
Although civilian “rescue societies” and ambulance services existed from the mid-1800s, the most significant nonmilitary advancement in EMS occurred in the 1950s with the establishment of life support training programs through the Chicago Fire Department. From this effort the basis for the now widely accepted emergency medical technician (EMT) and paramedic training programs were formed.2 By the 1960s, some regions had nascent ambulance systems with paramedics trained in advanced life support (ALS) techniques, although others developed a separate system of “heartmobiles” with physicians on board to provide care only for cardiac emergencies.7
The need for sophisticated, coordinated EMS systems was brought to the national spotlight in 1966 with publication of the National Academy of Sciences paper titled “Accidental Death and Disability: The Neglected Disease of Modern Society.” This paper noted that few people were trained in advanced resuscitation, no widely accepted standards had been established for training ambulance personnel, and communication systems and supplies were lacking. This report spurred a national, organized effort to increase awareness of traumatic disease and the need for development of a comprehensive EMS system.5 Congress responded with the National Highway Safety Act of 1966 and the EMS Systems Act of 1973, which authorized federal grants to state, local, and regional governments for the development of EMS systems within a specified “systems approach” framework.8 In 1981, however, guaranteed federal funding for EMS was replaced with state block grants and increased financial insecurity.4 Currently, nearly 1 million people are certified in some form as emergency response personnel, and nearly 20 million patients are treated in the EMS system annually, but heterogeneity in system design, scope, and certification requirements persists.9
EMS System Design
EMS systems are, arguably, some of the most complex organizational entities in modern society. They include representatives from municipalities of every size, law enforcement, fire and safety, health care, transportation services, and community groups. Federal governing bodies define the necessary components of EMS systems but do not directly oversee organization or management. Coordination between agencies is essential but often difficult to achieve.1 Ideally, EMS system design is centered around the particular needs of the community that it serves, with one standard characteristic: emergency medical personnel act as on-scene “physician surrogates” to provide appropriate life support techniques.7 Common models categorize different systems in terms of control by the public or private agencies, rural or urban communities, and single-tiered or multitiered systems.
Rural and Urban EMS Systems
The design of and challenges faced by EMS systems are often significantly different between rural and urban areas. In general, rural systems developed later than urban ones and are more likely to be staffed with unpaid volunteers.3 These volunteer-based organizations may be public or private and are generally nonprofit entities. Volunteers are usually citizens with outside employment who offer their services on an unpaid basis for emergency response, training, and community education. Funding is largely through taxes and municipal support, although private donations and fund-raising are often necessary. Volunteer EMS systems face many challenges that are representative of rural systems as a whole, namely, high cost to cover large geographic areas with few citizens, high response times, lower levels of training, and relatively low patient volumes.10,11 Urban EMS systems have their own distinct set of difficulties, among them high patient volumes, traffic congestion, and limited resources.
Evidence suggests that rural emergency morbidity and mortality is significantly greater than that for comparable urban patients. Reasons for this difference include longer response and scene times, lower patient volumes, and less overall training for first responders.12–15 Technologic advances such as “E911” (enhanced 911) show some promise in significantly reducing emergency responders’ transport time to the scene.16 Adapting specific on-scene protocols and increasing access to high-quality medical care (prehospital and in-hospital) in rural areas have also been suggested as possibilities to decrease the gap in rural-urban adverse outcomes.15
EMS System Organization, Training, and Transport Types
Dispatch and Medical Control
In the United States, 99% of the population has access to 911 for emergency calls.7 Most dispatch centers use E911, a system whereby the caller’s location is shown on the dispatch operator’s screen. Formal training for 911 dispatch personnel exists, and national guidelines that advocate for certification standards have been established.17 There is a trend toward consolidation of all emergency calls into one 911 center, where dispatchers take calls and then directly relay information to the appropriate EMS or public safety agency. Dispatch actions and instructions may be shaped by established guidelines that allow adaptation to the situation at hand or by more rigid protocols that detail a specific plan of action. Some agencies may rely on computerized algorithms to assist dispatch; a controlled trial of British nonurgent emergency calls found that using a computerized decision tool plus either nurse or paramedic input resulted in more than half the calls triaged as not needing an emergency ambulance. However, only 20% of these callers chose to cancel the ambulance, and this group had similar hospital admission rates as those triaged as needing emergency transport.18
EMS systems rely heavily on both online (direct) and off-line (indirect) medical control. Physician involvement in EMS medical control developed as physicians spent less time directly in the field and paramedics increased their training and ability to act as physician surrogates. Every EMS system is headed by a medical director, a physician with or without specialty training who has direct authority over operation of the system, performance of emergency personnel, and patient care. Standardized guidelines and requirements for EMS medical direction have been published by the American College of Emergency Physicians (ACEP).19,20
The evidence basis for improved patient outcomes with online medical control is mixed. It has been shown to significantly increase on-scene time, and orders given rarely deviate from existing protocols.21–23 However, there is some evidence that online medical direction may decrease the use of inappropriate resources while preserving outcomes in some patients.24 The greatest benefits of online direction may be in resolving difficult ethical or medicolegal situations on scene and in notifying receiving hospitals of incoming critical patients so that resources can be assembled and are ready before arrival of the patient.
Off-line medical direction refers to written protocols that guide common patient interactions, as well as continuing education and quality assurance initiatives. EMS systems have specific protocols for commonly encountered situations that, ideally, should improve patient outcomes and reduce time at the scene. Protocols should be developed on the basis of patient history, mechanism of injury, physiologic characteristics, local hospital capability, and transport times. Medical directors should be active in developing and implementing protocols, as well as in training responders in their application and quality evaluation of patient records.25 Research indicates that use of well-developed standing protocols significantly reduces on-scene time and decreases inappropriate treatment in the field.26 Furthermore, diagnostic accuracy plus agreement with physician assessment of patients is generally high.27
EMS Responder Personnel
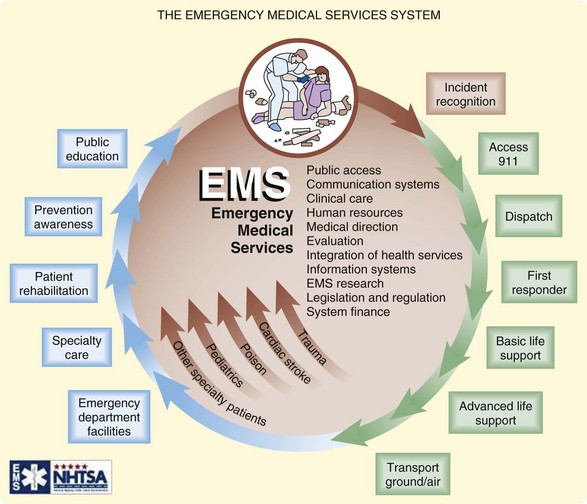
Before the National Academy of Sciences paper on trauma in the 1960s, few standardized training programs existed for EMS personnel. Subsequent creation of the Department of Transportation resulted in a formalized 70-hour curriculum for basic EMT certification. Passage of the EMS Systems Act of 1973 provided millions of dollars for EMS training, equipment, and research and identified basic elements that must be included in all EMS systems (Fig. 215.1).28 However, until recently, heterogeneity of regional systems persisted such that a 1996 survey identified more than 40 different types of EMS personnel certification across the country.29
Recognition of the wide regional variation in training standards and skill levels led to development of the National Highway Traffic Safety Administration National EMS Scope of Practice Model in 2005. This consensus document promotes national standardization in training and education to improve consistency within and among agencies, increase public understanding of EMS roles, and move toward a coordinated national EMS system.9 The model advocates four separate and sequential levels of certification—emergency medical responder, EMT, advanced EMT, and paramedic—and clearly defines minimum educational levels and skill sets for each. Most states have already implemented or are in the process of testing these national guidelines for local use.
There is some evidence basis for the current multilevel EMS personnel system. Early EMS research found a significant reduction in mortality from cardiac arrest with the use of paramedic responder crews versus EMT-Bs.30,31 Outcomes in trauma have also been shown to improve significantly when ALS-capable ambulances are on scene as compared with BLS personnel.32,33 However, other studies evaluating paramedic- and non–paramedic-containing crews found mixed results. In general, on-scene time is significantly longer for crews in which one or all of the responders are paramedics.34,35 Paramedic crews had higher skill levels and provided more on-scene interventions, but some authors suggest that their presence on every ambulance may not be warranted.36
EMS Vehicles, Equipment, and Types of Transport
Equipment available on emergency transport vehicles varies by both type of vehicle and the skill level of responder personnel on board. Joint guidelines developed by the ACEP and the American College of Surgeons detail the minimum necessary supplies for appropriate patient care.36 Items needed for basic-level interventions include ventilation and airway equipment, monitors and defibrillators, immobilization devices and bandages, mobile communication devices, obstetric and pediatric specialty equipment, and infection control and injury prevention measures. Ambulances with advanced life support capability (EMT-I or EMT-P) should contain all the aforementioned basic equipment plus vascular access material, advanced airway and ventilation tools, advanced cardiac life support and other protocol-driven medications, more sophisticated monitoring, and advanced diagnostic equipment (e.g., glucometer, pulse oximeter). In addition, all vehicles should have some measure of extrication equipment for use in patient rescue.
Air Medicine Transport
Although a full description of air ambulance systems is beyond the scope of this chapter, this method of transportation plays a crucial role in the transport and transfer of critically ill patients. Ground emergency transport remains the mainstay of prehospital transport and transfer; however, air medical services can have a significant impact on patient care in selected conditions.37,38 The benefits of air ambulance transport are largely attributed to increased speed and higher crew skill levels; however, safety, cost, and limited evidence to support improved outcomes are major concerns.
The literature on selected prehospital air transport focuses largely on trauma patients and presents mixed evidence for its use. Retrospective evaluations of trauma patients have shown a significant decrease in mortality with helicopter transport39,40; however, several studies have found no difference in patient outcomes for both trauma and nontrauma conditions36–38 and that air transport is overused and costly.40–44 Criteria for air transport can vary widely by EMS system, and overtriaging is common.45
The National Association of EMS Physicians has published guidelines regarding the use of various methods of air transport, as well as which patients are most likely to benefit from its use. In general, helicopters are best used for transport involving a shorter distance (less than 100 miles) but are subject to weather concerns. Fixed-wing aircraft are preferable for distances greater than 100 miles and are less dependent on inclement weather, but they must land at airports (thereby prolonging transport time). Severely injured trauma patients at some distance from a regional trauma center are most likely to benefit from air transport or transfer; critically ill nontrauma, cardiac, pediatric, and possibly obstetric patients may also have improved outcomes in selected situations.46
The safety of both patients and medical staff is a prominent issue in air medical transport. As the number of flights has increased in recent years, so has the number of aircraft accidents. Between 2002 and 2005, 55 crashes occurred and resulted in 54 fatalities; the incidence of aircraft accidents per number of flights increased as well.47 Patient safety in flight is also of concern; an estimated 5% of patients suffer a “critical event” (decompensation or deterioration) during transport.45 Factors such as weather, time of the day, terrain, communication difficulties, and medical crew training have been found to be associated with adverse events, but more study is needed to improve air transport safety.







