(1)
Chennai Breast Centre, Chennai, India
Ductal carcinoma in situ is a malignant proliferation of epithelial cells within the ducts with no invasion. DCIS (ductal carcinoma in situ) is a heterogenous group of lesions that have very different morphology, biology, and clinical behavior. It is considered to be a true precursor of invasive disease although not all DCIS progress to become invasive carcinoma.
Prior to breast cancer screening, DCIS was seldom seen. DCIS accounts for a quarter of cancers detected on population-based breast cancer screening. Majority of these will be nonpalpable lesions. Some women may present with a palpable mass, nipple discharge, or as Paget’s disease.
Based on the morphology, DCIS was conventionally classified as cribriform, comedo, micropapillary, and solid-type DCIS. However, individual lesions often show a mixed architecture. More recently DCIS is now being categorized based on nuclear grade and necrosis into low, intermediate, or high-grade DCIS. The Van Nuys Classification system for DCIS proposed by Silverstein et al in 1994 identifies three groups based nuclear grade and necrosis. Group one includes lesions with non-high-grade DCIS without necrosis. Group 2 includes non-high-grade DCIS with necrosis. Group 3 includes high-grade DCIS with or without necrosis.
High-Grade DCIS
High-grade DCIS is characterized by presence of pleomorphic cells with increased mitoses. As the cells proliferate within the lumen, the central cells undergo necrosis and calcify. Hence high-grade DCIS is often screen detected and diagnosed by the presence of microcalcifications on mammograms (Fig. 30.1).
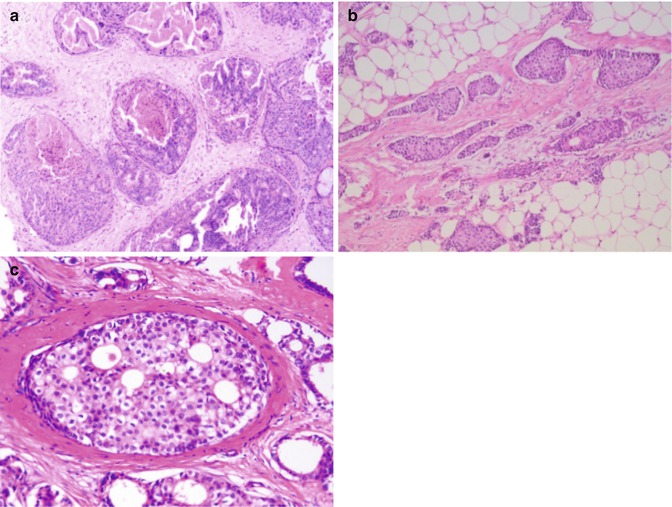
Fig. 30.1
(a) High-grade solid DCIS with central comedonecrosis. Cells are markedly pleomorphic with vesicular nuclei and prominent nucleoli. (b) Low-power view of low grade DCIS: several ducts completely filled by relatively monomorphic cells with rounded nuclei. (c) High power: duct filled by cells with nuclei two to three times that of RBC, with sharply punched out holes (cribriform pattern); no comedonecrosis
Low-Grade DCIS
Low-grade DCIS is characterized by the presence of small, regular cells, with round nuclei. Mitoses are infrequent. They may have micropapillary or cribriform architecture. Occasionally, they may have a solid architecture. The cells lining the micropapillae or the lumen show polarization.
Atypical ductal hyperplasia is close to low-grade DCIS in appearance. If the cellular features typical of low-grade DCIS occupy more than two duct spaces, it is termed low-grade DCIS and if it less than two duct spaces it is generally called atypical ductal hyperplasia.
Intermediate DCIS
Intermediate-grade DCIS is characterized by cells with moderate nuclear pleomorphism, but lack the regularity of the size and spacing of the low-grade DCIS. Some degree of polarization is often present. When a lesion cannot be categorized into a low- or high-grade DCIS, they are usually called as intermediate-grade DCIS.
When there are mixed grades within the same lesion, then the highest grade should be recorded.
DCIS (Special Types)
Encysted papillary DCIS is often seen in older women, and is usually palpable and well circumscribed. Papillary architecture with fine fibrovascular core is seen. Immunohistochemistry for smooth muscle myosin heavy chain or smooth muscle actin reveals the absence of a myoepithelial layer.
Paget’s Disease
Paget’s disease was described by Sir. James Paget in 1984 as “an eczematous change in the skin of the nipple preceding an underlying mammary cancer”. Majority of women with Paget’s disease will have an underlying invasive or in situ malignancy.
Paget’s disease starts in the nipple and spreads to the areola. Patients may complain of burning sensation or itching initially. The skin over nipple and areola is usually thickened with scaling and erythema. In the latter stages, the nipple ulcerates and spread to the areola. Chronic eczema resembles Paget’s disease closely and a full thickness biopsy of the nipple should be performed to confirm the diagnosis. Mammography may show an underlying mass or calcification with thickening of nipple and areola. In early stages, mammography might be entirely normal. Histologically, they have a characteristic appearance. Paget’s cells appear as large, round, or ovoid intraepithelial cells with abundant pale cytoplasm and pleomorphic and hyperchromatic large nuclei.
Paget’s with an invasive component is treated like an invasive malignancy. Paget’s with no invasive component is treated with mastectomy or local excision with regional flaps followed by radiotherapy.
Mammographic Features
The hallmark of DCIS on mammograms is calcifications. They are seen in nearly 90 % of the patients with DCIS. Calcifications in DCIS can arise due to different mechanisms.
Three main patterns of calcifications are recognized with DCIS.
1.
Fine, linear branching calcifications
2.
Irregular pleomorphic calcifications
3.
Indistinct, amorphous calcifications
Fine Linear Branching Calcifications
The ductal lumen is filled with the high nuclear grade cancer cells which outgrow the blood supply in the center and undergo necrosis in the centre. The necrotic debris calcifies producing the fine, irregular, linear branching calcifications (V and Y forms) that take the outline of the duct and its branches. They appear like casts of the ducts and hence called by Dr. Tabar as casting-type calcifications. The presence of this type of calcifications is highly suggestive of a high nuclear grade carcinoma with necrosis (Van Nuy’s group 3) (Figs. 30.2, 30.3a, b, 30.4, 30.5, and 30.6)
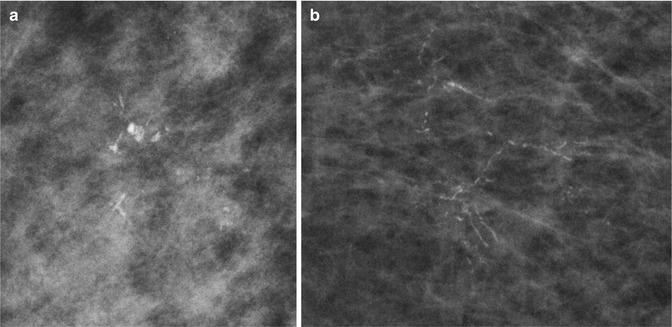
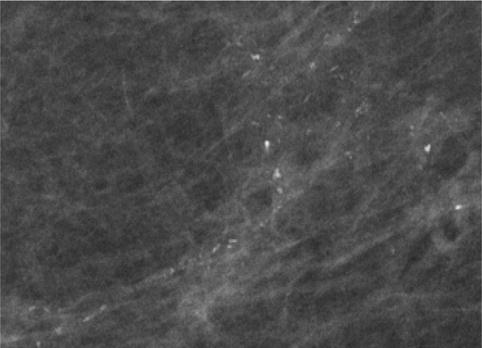
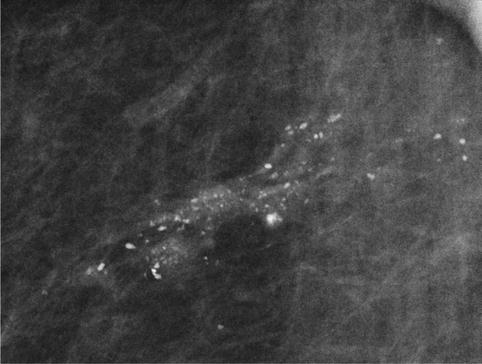
Fig. 30.2
Schematics showing ductal anatomy
Fig. 30.3
(a, b) Magnified mammographic images showing fine, irregular, linear calcifications with V and Y forms taking the outline of the duct and its branches. HPE: high-grade DCIS
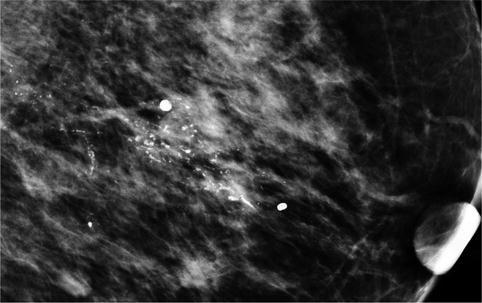
Fig. 30.4
Fine linear branching calcifications. HPE: high-grade DCIS
Fig. 30.5
Fine irregular, pleomorphic calcifications in a linear distribution