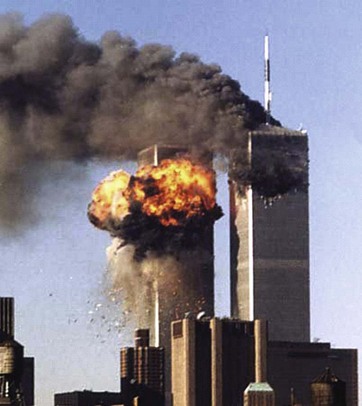
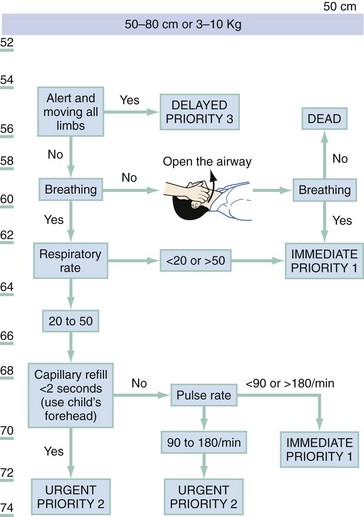
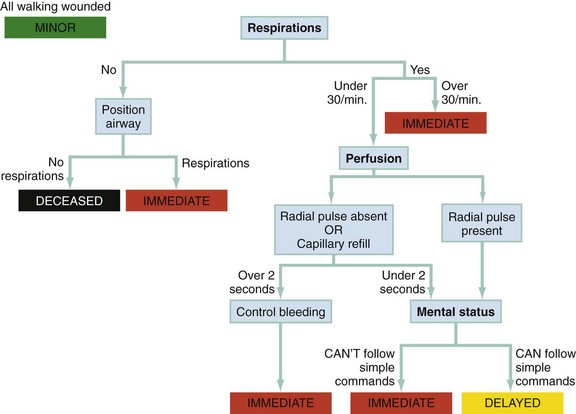
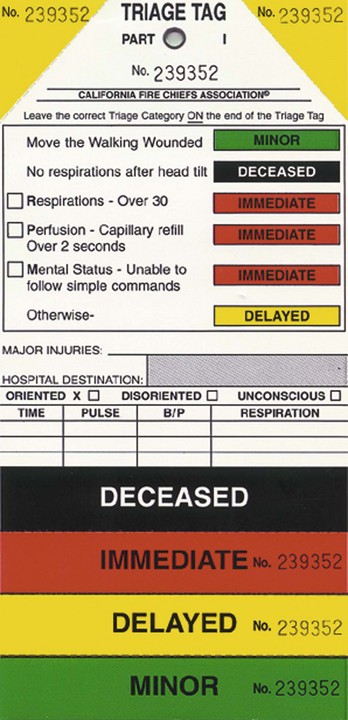
Chapter 193 Disasters occur in all areas of the world and cause harm to people, property, infrastructures, economies, and the environment. Harm to people includes death, injury, disease, malnutrition, and psychological stress. Recent catastrophes include earthquakes in Pakistan (2005) and Haiti (2010) (Fig. 193-1); devastating tsunamis in the Indian Ocean (2004) and Japan (2011); massive hurricanes in the southern United States (2005); severe flooding in Australia (2011); tornadoes in Arkansas, Tennessee, and Kentucky (2008); and unusual weather conditions producing record snowfalls in the United States and Europe (2011). Increasing population density in floodplains and in earthquake- and hurricane-prone areas and the effects of global warming point to the probability of future catastrophic disasters with large numbers of casualties. Given this probability and the increasing role of emergency medicine in disaster preparation, mitigation, response, and recovery, this chapter discusses disaster planning and operations with emphasis on the role of the emergency physician. The emergency physician has extensive responsibilities for community disaster preparedness and disaster medical services, including response to terrorism. In position and policy documents, the American College of Emergency Physicians outlines the scope of emergency medicine’s involvement in preparedness and response to disasters and terrorism, stating that “emergency physicians should assume a primary role in the medical aspects of disaster planning, management, and patient care” and that “emergency department personnel will become the first responders to a covert biological attack.”1,2 A committed emergency department alone is insufficient to provide hospitals with a successful disaster preparedness program. Institutional commitment by every hospital department and the administration is necessary to coordinate effectively with system-wide resources for disaster management. This is especially critical for creation of hospital surge capacity.3–5 A partial listing of general disaster medicine resources can be found in Table 193-1. Table 193-1 List of Disaster Medicine Resources The concept of surge capacity has emerged as a way to manage an event that produces a sudden influx of casualties with medical and health needs that exceed current hospital resources.6 This can be due to either the volume or types of victims. The three basic components of the surge capacity system are commonly referred to as the three s‘s of staff (hospital personnel), stuff (supplies and pharmaceuticals), and structure (physical location and management infrastructure). A complete discussion of surge capacity is beyond the scope of this chapter but has been published elsewhere.7 Some definitions have been based on the number of casualties. As previously described, the absolute number of patients is much less important than whether their medical and health needs exceed the resources to care for them at a given point in time. Another historical scheme divides disasters into three levels. Level I denotes a situation in which local resources are adequate to care for casualties. For example, the 2002 collision between a freight train and commuter train in Orange County, California, was managed effectively by local responders. Level II means that regional mutual aid is required to respond to the event. This was the case at the Hyatt Regency Hotel in Kansas City in 1981 when two skywalks collapsed, killing 114 people and injuring hundreds. Level III incidents require state and federal aid. The attack on the World Trade Center in 2001 (Fig. 193-2) and hurricane Katrina in 2005 were such events, causing such massive destruction that federal disaster medical assistance teams were deployed to New York and Louisiana, respectively, to provide medical personnel and supplies. Figure 193-2 The World Trade Center attack of 2001 overwhelmed local resources and necessitated state and federal help. One model eliminates the word disaster and replaces it with the acronym for potential injury-creating event, PICE.8–10 The PICE nomenclature is an attempt to resolve the issue regarding diverse meanings for disaster. This model is referenced in the Joint Commission standards and in publications from several countries. The PICE system is discussed here to help clarify important concepts in describing an event. The acronym PICE and its modifiers concisely describe the critical features of most types or degrees of disaster.8–10 The same occurrence can have different effects at different points in time; thus, as an event evolves over time, its description may change. Modifiers are chosen from a standardized group of prefixes along with a stage to indicate the need for outside medical assistance (Table 193-2). The first prefix (column A) describes the potential for additional casualties. The second prefix (column B) describes whether local resources are overwhelmed and, if so, whether they must simply be augmented (disruptive) or whether they must first be totally reconstituted (paralytic). The third prefix (column C) shows the extent of geographic involvement.8–10 Column C refers strictly to the affected region and not to the location that sends assistance. Rather, the “stage” rating scale defines the likelihood that outside medical assistance will be needed either to augment or to completely reconstitute resources.8 Stage 0 means that there is little or no chance. Stage I means that there is a small chance and requires placing outside medical help on alert. Stage II means that there is a moderate chance and outside help should be placed on standby. Stage III means local resources are clearly overwhelmed and require the dispatch of outside resources and commitment of personnel. For example, a multivehicle collision with a dozen injuries and several deaths in a large city would be a stage 0, whereas in a small rural town it might be a stage III (Table 193-3). Table 193-3 A PICE can be either static or dynamic. Dynamic implies an evolving situation in which it is too soon after the incident to determine the numbers and types of casualties and the impact on the hospital. Alternatively, a static situation results if 10 people are injured in an incident and little potential for further harm exists.8–10 In some situations, enhancement of routine operations is not sufficient or possible. A PICE can completely overwhelm the capability to mount a normal response so that a substitute plan for recovery must be used. Situations that require significant reconstitution of critical resources are termed paralytic.8–10 Within the hospital, there are six critical elements necessary to provide a response (Box 193-1).11 If one or more of these resources are compromised, they must be reconstituted or a substitute must be implemented. Such paralytic events can be either destructive or nondestructive (Box 193-2).8 After performing a hazard vulnerability analysis (www.emsa.ca.gov/disaster/files/kaiser_model.xls), emergency planners should consider the most probable events and prepare for them. There should also be planning for events that are rare but catastrophic.12 The major peacetime threat to life and limb in the United States is probably a large earthquake in a densely populated area or a terrorist attack. The disaster planner should proactively identify all such hazards and prepare contingency plans for each. The term triage derives from the French verb trier, meaning “to sort.” The concept of triage was used as far back as Napoleon’s time to assign priorities to treatment of the injured when resources were limited. Priority is given to the most salvageable patients with the most urgent conditions. The emergency department uses triage in the hospital setting on a daily basis, but the focus of such triage is changed under disaster conditions.13,14 Standard emergency department triage is intended to identify the most seriously ill patients first and to ensure that they receive rapid care. The goal of disaster triage is slightly different, that is, “to do the most good for the most people.” In other words, there is a shift from focus on individual patients to focus on the entire affected population.15 It can be difficult for physicians to realize that to achieve the goal of maximizing benefit to an entire population of patients, they may need to let some patients die with only comfort care. Under true disaster conditions, cardiopulmonary resuscitation should not be performed.16 To assist in understanding of triage techniques, it is useful to consider a routine out-of-hospital event with multiple casualties (e.g., a multivehicle collision). In such situations, rescue personnel often use a Simple Triage and Rapid Treatment (START) technique that depends on a quick assessment of respiration, perfusion, and mental status.17 These three assessments can be remembered by the mnemonic RPM (respirations, perfusion, and mental status). Initially, all victims who are able to walk are asked to move away from the immediate incident area. These patients are classified as green, or “walking wounded,” and are reassessed after the more immediately critical patients are triaged. The Pediatric Triage Tape (PTT) and JumpSTART have been proposed for the triage of children. JumpSTART is a modification of the START triage protocol that includes an additional step of five rescue ventilations for children presenting apneic and modification of criteria for hypoventilation and tachypnea as well as for a decrease in mental status. The PTT uses criteria that change in proportion to increasing victim size. The parameters for a child 50 to 80 cm in length are illustrated in Figure 193-3. In a comparison of sensitivity and specificity between the PTT and JumpSTART in pediatric trauma patients, the PTT demonstrated superior outcomes.18 Both START and the PTT appear to be useful tools, but only START has been evaluated in an actual disaster situation.19–21 As illustrated in Figure 193-4, a rescuer can assess each patient in seconds, quickly checking respiratory rate, pulse, and ability to follow commands (mental status), and divide the patients into the remaining three categories: red (immediate), yellow (delayed), and black (deceased). The only patient care interventions provided during this process are the opening of an obstructed airway and direct pressure on obvious external hemorrhage. At this point, patients are generally transported to a hospital for definitive care. Most often, patients arrive with a color-coded triage tag and are reassessed and retriaged by the hospital staff (Fig. 193-5). An outcomes-based evaluation of the performance of START triage in an actual disaster (2002 Placentia Linda train crash) demonstrated acceptable levels of undertriage (100% sensitivity of the red category and 90% specificity of the green category).21 However, significant amounts of overtriage occurred. Use of START also appropriately prioritized the transport of victims, with patients triaged as red arriving at hospitals earlier than patients triaged as yellow or green. Recently, a multidisciplinary group was formed to propose a potential national triage system for the United States. The result, derived by consensus of opinions, was referred to as SALT (sort, assess, lifesaving interventions, and treatment or transport).22 It differs from START mainly in the assessment of respirations (relies on a qualitative evaluation of respiratory distress rather than a number), the requirement for performance of certain emergent interventions (chest decompression), and an unstructured estimate of survivability. The algorithm is more complicated than START, and no current data exist evaluating its sensitivity, specificity, or other performance characteristics in a disaster. As such, it is not currently possible to make recommendations for its use. To address this situation, researchers developed the Secondary Assessment of Victim Endpoint (SAVE) system of triage.23 The SAVE triage system is designed to identify patients who are most likely to benefit from care available under austere field conditions in a resource-poor environment. When it is combined with the START protocol, SAVE triage is useful for any scenario in which multiple patients experience a prolonged delay in accessing definitive care. The SAVE triage methodology divides patients into three categories: (1) those who will die regardless of how much care they receive, (2) those who will survive whether or not they receive care, and (3) those who will benefit significantly from austere field interventions. Only those patients expected to improve receive care beyond basic and comfort measures. With use of SAVE, patients are separated into these three categories so resources can be focused appropriately. The decision to place patients in a particular group is based on field outcome expectations derived from existing survival and morbidity statistics.23 An example is a situation in which three victims require chest tubes (two victims require one tube each and one victim requires two tubes), but only two chest tubes are available. The SAVE principles guide providers to place their last two chest tubes into the two victims who need it rather than into the single victim requiring two tubes. Since nuclear, biologic, and chemical terrorism has become a threat, new triage systems are under development.13,24 These systems attempt to incorporate the added threats from exposure and contamination into the triage process. One such method for biologic casualties triages many individuals to home observation rather than hospitalization to optimize resource use and to minimize the spread of the infectious agent.24 In addition, responders must be protected from secondary contamination or exposure; therefore, part of the triage algorithm should include a risk assessment and determination of whether and what type of personal protective equipment should be donned before patients are assessed. A quick determination is critical to prevent patient deaths from traumatic injuries while awaiting medical care from responders concerned about their own health and safety. This is particularly true in a “combined event” scenario, such as an event involving a radiologic dispersion device. Also associated with terrorism incidents are large numbers of psychogenic casualties, those who believe they were exposed but actually were not and those at risk for post-traumatic stress disorder. The emergency plan should include a mechanism to assess and to sort these individuals so as not to overwhelm the emergency department and also provide mental health care. While performing triage, the emergency physician should also consider the effects of extremes of age, underlying disease, and multiple injuries when assessing the potential prognosis for a given patient. Fortunately, the treatment of many nontraumatic emergencies can be accomplished with field interventions that do not consume extensive resources. Therefore, patients with such illnesses should usually be triaged to the treatment area.
Disaster Preparedness
Perspective
ORGANIZATION
WEBSITE
The Joint Commission
www.jointcommission.org/
American College of Emergency Physicians
www.acep.org
Centers for Disease Control and Prevention, Emergency Preparedness and Response
www.bt.cdc.gov/training/
FEMA National Preparedness Directorate, National Training and Education
http://training.fema.gov/
National Response Framework
www.fema.gov/emergency/nrf/
Agency for Healthcare Research and Quality
http://archive.ahrq.gov/prep/
Koenig and Schultz’s Disaster Medicine: Comprehensive Principles and Practices
Cambridge University Press
www.cambridge.org
Surge Capacity
Nature of Disasters
Classic Terminology
Potential Injury-Creating Event Nomenclature
World Trade Center attack, September 11, 2001
Dynamic, paralytic, local, PICE stage III
Los Angeles civil disturbance
Dynamic, paralytic, regional, PICE stage I
Northridge earthquake
Dynamic, disruptive, regional, PICE stage II
Oklahoma City bombing
Dynamic, disruptive, local, PICE stage I
Hazard Vulnerability Analysis
Triage
Routine Multiple-Casualty Triage
Catastrophic Casualty Management
![]()
Stay updated, free articles. Join our Telegram channel







Full access? Get Clinical Tree


