116 Dialysis-Related Emergencies
 Key Points
Key Points• Infection is a common cause of morbidity and mortality in dialysis patients. Tunneled lines and temporary dialysis catheters are more likely to become infected than grafts and native arteriovenous fistulas.
• The differential diagnosis of hemodynamic instability in a hemodialysis patient is dependent on the associated signs or symptoms (e.g., fever, chest pain), as well as the duration and speed of onset of the instability.
• Early vascular surgery consultation is necessary for patients with clotted hemodialysis access.
• Peritonitis is a common infection associated with peritoneal dialysis. Turbidity is one of the earliest signs of infection.
• Empiric treatment of peritoneal dialysis–associated peritonitis should include intraperitoneal antibiotics with both gram-positive and gram-negative coverage.
Scope
In the United States, in excess of 380,000 patients with renal failure rely on some form of dialysis as life-sustaining renal replacement therapy. More than 90% of these patients are managed with hemodialysis, whereas about 7% use peritoneal dialysis (PD).1 The most common complication associated with either dialysis modality is infection, although many access site malfunctions and dialysis-related emergencies prompt visits to the emergency department (ED) by this population.
Hemodialysis
Structure and Function
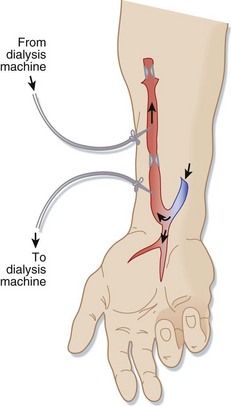
Connecting an artery (usually in the forearm) directly to a vein via surgery creates a native AV fistula (Fig. 116.1). Over months, the increased blood flow creates a larger, stronger vein with adequate blood flow for dialysis. Native AV fistulas are less likely than other forms of hemodialysis access to become infected or form clots.
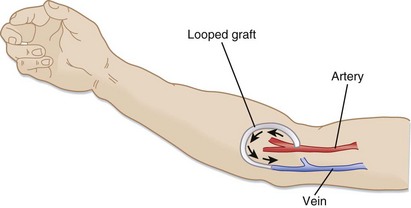
Synthetic AV grafts (Fig. 116.2) are used when forearm veins are unsuitable for native grafts. Synthetic grafts can be used within weeks of placement; however, they have higher infection and clotting rates than native AV fistulas do.
Central venous catheters (Fig. 116.3) are used when dialysis access is needed before permanent AV grafts have had time to mature or when fistula or graft surgery fails. Approximately 25% of the hemodialysis patients in the United States use central venous catheters as their primary vascular access. Tunneled, cuffed catheters have a lower infection rate than nontunneled catheters do. All these catheters have a double lumen and are at higher risk for infection and clotting than AV fistulas or grafts are.

Complications
Infection
Infectious complications are among the foremost causes of morbidity and mortality in hemodialysis patients. The risk for infection results from both impaired immune function related to the renal failure (e.g., altered granulocyte function in uremia) and repetitive access of the vasculature across the protective skin barrier. Vascular access is the source of bacteremia in 48% to 73% of infected hemodialysis patients.2
Clinical findings may include fever, hypotension, altered mental status, skin infection at the access site, and severe sepsis. Patients with diabetes may have ketoacidosis. The differential diagnosis of the various clinical findings in hemodialysis patients is described in Table 116.1.
Table 116.1 Differential Diagnosis of Various Clinical Findings in Hemodialysis Patients
Removal or exchange of an infected catheter is advisable because a bacterial biofilm can form rapidly in the lumens of most indwelling central venous catheters and serve as a source of continued infection. Systemic antibiotics given alone are relatively ineffective in eradicating infection if the catheter is not removed. There are occasional protocols that have demonstrated catheter salvation, but none have done so reliably. Catheter removal with delayed replacement is required in patients who are clinically unstable, who have metastatic infectious complications, or who have tunnel infections.3 Tunneled catheters can be replaced with temporary nontunneled catheters or can be changed over a guidewire, thus avoiding disruption of the patient’s dialysis schedule.
Thrombosis
Thrombosis of hemodialysis access grafts and catheters is a significant cause of morbidity. Failure of hemodialysis grafts is mainly due to progressive intimal hyperplasia at the venous anastomosis and resultant decreased flow and graft thrombosis.4
Thrombolytic agents can be initiated in consultation with a vascular surgeon. Several different thrombolytic regimens can be used. One protocol involves the use of 2 to 4 mg of alteplase infused through an 18- to 22-gauge intravenous line while waiting for the availability of angiography. If the wait time exceeds 30 minutes, an additional 2 mg is given.5 Care must be taken to confirm that the intravenous tubing has actually been inserted into the graft pointing toward the occlusion and not into surrounding tissue or another vessel before infusion of the thrombolytic agent. The arterial limb of the graft should also be occluded while the thrombolytic agent is being infused.
Bleeding
Hemodialysis patients are at risk for hemorrhage from other sites because of anticoagulation during dialysis. Platelet dysfunction secondary to uremia also contributes to hemorrhage in patients with renal failure, and it is only partially corrected by hemodialysis. Administration of desmopressin (DDAVP) (0.3 mcg/kg intravenously with 50 mL saline over a 3-minute period, 0.3 mcg/kg subcutaneously, or 2 mcg/kg intranasally) improves the hemostatic function of platelets and is useful in treating hemorrhage in hemodialysis patients. The maximal effect of DDAVP occurs after 1 hour, and if immediate hemostasis is needed, 10 units of cryoprecipitate can be infused over a 30-minute period.4
Pseudoaneurysm
Pseudoaneurysms are more likely to occur with prosthetic grafts, but they can also develop with autogenous access. Duplex ultrasound can be used to distinguish between pseudoaneurysms and other perigraft fluid collections. Small puncture site pseudoaneurysms can sometimes be monitored, but pseudoaneurysms at the anastomosis of the graft require surgical or endovascular revision and are often associated with infection. Vascular surgery consultation is necessary for suspected pseudoaneurysms.4
Dialyzer Reactions
Patients undergoing their first hemodialysis session or those switching to a new dialyzer may experience anaphylaxis or an anaphylactoid reaction to a component of the dialyzer or dialysate. Anaphylactoid reactions have been observed with dialyzers made of cuprophane and with polyacrylonitrile dialysis membranes (particularly in patients taking angiotensin-converting enzyme inhibitors). Treatment consists of epinephrine, antihistamines, and steroids.6
Tips and Tricks
Use of Hemodialysis Graft or Catheter for Emergency Vascular Access







