Chapter 24 Diagnostic and Therapeutic Cardiac Catheterization
Catheterization Laboratory Environment
Safe transportation of a critically ill child from the intensive care unit to the catheterization laboratory can be a significant challenge but should not be a deciding factor as to whether or not the procedure should be performed. Safe transport requires planning and multidisciplinary coordination. This process includes physician and nursing staff accompanying the patient with complete monitoring and resuscitation equipment, respiratory therapy staff to assist with ventilation and establishing mechanical ventilation in the catheterization laboratory if indicated, coordinating timing with the catheter laboratory staff to prevent needless delays, assistance with establishing adequate space for equipment and patient access in the laboratory, and correct positioning on the catheterization table to enable access for both the catheterizer and intensive care staff as necessary.
Adequate sedation and anesthesia during cardiac catheterization are essential to facilitate acquisition of meaningful hemodynamic data and to assist during interventional procedures. For the most part, hemodynamic or diagnostic catheterization procedures can be performed with the patient under sedation.1 For many interventional procedures, sedation may be appropriate; however, for procedures that are associated with significant hemodynamic compromise or are prolonged, general anesthesia is preferable. Whatever technique is used, hemodynamic data must be attained in conditions as close to normal as possible. For accurate calculation of the intracardiac shunt, reducing the inspired oxygen concentration to room air may be necessary, although this step requires close collaboration with the catheterizer because lowering FiO2 may be inadvisable in patients with significant desaturation and lung injury.
Hemodynamic and Oxygen Saturation Data
Hemodynamic cardiac catheterization may not be necessary when echocardiographic analysis with Doppler measurements and color flow mapping is complete and unambiguous. However, in patients with complex cardiac anatomy, severe low cardiac output state, pulmonary hypertension, severe lung injury of uncertain etiology, or with concerns for important residual anatomic lesions after cardiac surgery, physiologic data from catheterization may provide important information.2 Catheterization allows description of the direction, magnitude, and approximate location of intracardiac and intrapulmonary shunts. Intracardiac and intravascular pressures are measured to determine the presence of obstructions and whether shunt orifices are restrictive or nonrestrictive. Pressure gradients across sites of obstruction must be considered in light of estimated cardiac output, as a small pressure gradient measured at a time of low cardiac output is misleading.
Normally, no significant change in oxygen saturation from venae cavae to pulmonary artery is observed. In the child with congenital heart disease, the superior vena cava provides the simplest mixed venous oxygen saturation. A greater than 5% to 10% increase in oxygen saturation from the superior vena cava through to the pulmonary artery suggests the presence of a left-to-right shunt at the level of the right atrium with an atrial septal defect (ASD), in the right ventricle (RV) with a ventricular septal defect (VSD), and in the pulmonary artery with a patent ductus arteriosus (PDA) or aorto-pulmonary artery collateral vessels.3 The magnitude of the left-to-right shunt can be calculated by applying the Fick equation to the pulmonary and systemic vascular beds separately (assuming O2 uptake and consumption are equal):


where Qp is pulmonary blood flow, Qs is systemic blood flow, VO2 is oxygen consumption, SpvO2 is pulmonary vein saturation (which can be assumed to be 0.96 in the absence of significant pulmonary disease), SpaO2 is pulmonary artery saturation, SaO2 is arterial oxygen saturation, SsvcO2 is superior vena cava oxygen saturation, and Hb is hemoglobin. (Note that saturation data in the equations is expressed as a decimal number and not as a percentage, e.g., 98% saturation = 0.98.)
In pediatric patients, the pulmonary and systemic flows usually are indexed to body surface area:

where CI is cardiac index and BSA is body surface area.
Thermodilution can be used to calculate the cardiac output in pediatric patients, although it is confounded by the presence of intracardiac or extracardiac shunts.4 Although measurement of oxygen consumption is preferable5 because assumed values are unreliable in patients with critical illness and in those requiring substantial hemodynamic support, the practical reality is that the majority of catheterization laboratories tend to assume oxygen consumption.6 The inherent error of all calculations should always be considered, particularly with respect to flow and resistance calculations.
The pulmonary to systemic blood flow ratio (Qp/Qs) can be derived simply from the measured oxygen saturation values because all other variables cancel out (from Equations 1 and 2):

Vascular resistance is calculated by the change in pressure divided by the flow (Dp/Q):
Pulmonary vascular resistance (PVR) =

Systemic vascular resistance (SVR) =

where PAP is pulmonary artery pressure, LAP is left atrial pressure, AoP is aortic pressure, SVCP is superior vena cava pressure, Qp is pulmonary blood flow, and Qs is systemic blood flow.


Assessment of Critical Illness
The cardiac catheterization laboratory can be useful in a number of situations during the management of critically ill infants and children who have structurally normal hearts (Table 24-1) or congenital heart disease. Fluoroscopy can be used to assist with placing difficult central venous or pulmonary artery lines, performing pericardiocentesis and pleurocentesis, and assessing diaphragm function.
Table 24–1 Indications for Cardiac Catheterization or Management in the Catheterization Laboratory of Pediatric Intensive Care Patients with Noncongenital Heart Disease
| Diagnostic | |
| Therapeutic |
Patients with pulmonary hypertension can benefit from investigation in the catheterization laboratory. Catheterization may help diagnose or rule out structural disease involving the pulmonary arteries or pulmonary veins, as in cases of multiple thromboembolic disease or undiagnosed pulmonary vein stenosis. Data obtained during catheterization are important for evaluation of the response of pulmonary vasculature to vasodilator treatment, for example, with increased FiO2 or inhaled nitric oxide.7 Such evaluation and measurement of a specific response is important for longer-term management strategies of patients with pulmonary hypertension. In the presence of a left-to-right shunt and elevated PVR, pressure and saturation measurements often are repeated with the patient breathing 100% oxygen to assess both the reactivity of the pulmonary vascular bed and any contribution of ventilation/perfusion abnormalities to hypoxemia. If breathing 100% oxygen and inhaled nitric oxide increases pulmonary blood flow and dramatically increases Qp/Qs (with a fall in PVR), potentially reversible processes such as hypoxic pulmonary vasoconstriction may be contributing to the elevated PVR. The patient with a high, unresponsive PVR and a small left-to-right shunt may have extensive pulmonary vascular damage from the underlying lung injury or irreversible obstructive pulmonary vascular disease.
Patients who present with severe cardiac failure because of myocarditis or idiopathic dilated cardiomyopathy or intractable dysrhythmias often require cardiac catheterization, not only for hemodynamic assessment but also for endomyocardial biopsy. Biopsies in these circumstances can be associated with significant morbidity, and treatment of the baseline condition should not be delayed until catheterization is performed.8,9 The risk of myocardial perforation is particularly increased in infants with thin-walled ventricles, and biopsy should be reconsidered in infants with a very dilated and poorly functioning left ventricle. Patients who have a low cardiac output state associated with fulminant myocarditis are at risk for dysrhythmias during catheterization, and resuscitation resources must be immediately available, including mechanical support. The catheterization study and desire for a biopsy in an effort to establish a diagnosis must not take priority over efforts to support the circulation and maintain cardiac output.
Transcatheter Radiofrequency Ablation
Pediatric patients undergoing radiofrequency catheter ablation (RFCA) vary in age and diagnosis.10 Ablation may be necessary in newborns or infants with persistent reentrant tachycardia or ectopic atrial tachycardia11,12 and in older children with ectopic foci but otherwise structurally normal hearts that are refractory to or poorly controlled by conventional antiarrhythmic drugs. If an incessant dysrhythmia, particularly a supraventricular tachycardia such as ectopic atrial tachycardia or permanent junctional reciprocating tachycardia, is the primary cause of a dilated poorly contracting heart at the time of presentation, electrophysiologic study and mapping of the dysrhythmia focus may be important diagnostic steps performed in the catheterization laboratory. Elective mechanical support of the circulation with extracorporeal membrane oxygenation (ECMO) may be indicated in order to preserve hemodynamic stability during ablation.13 Successful RFCA in this circumstance may enable recovery of ventricular function.14
An increasing population of patients undergoing ablation consists of those with previous surgical repair of congenital heart defects. Patients with persistent volume or pressure load on the right atrium and those who required an extensive incision and suture lines within the right atrium, such as following a Mustard, Senning, or Fontan procedure, may be at increased risk for supraventricular tachyarrhythmias (SVT) such as atrial flutter and fibrillation.15,16 Ventricular tachyarrhythmias may develop late after repair of certain congenital heart defects, such as right ventricular outflow tract reconstruction for tetralogy of Fallot.17
On occasion, holding ventilation in either inspiration or expiration may be necessary to ensure adequate contact of the ablation catheter with the arrhythmic focus. For the most part, RFCA procedures are well tolerated hemodynamically and blood loss is minimal. During mapping, the focus is stimulated and the tachyarrhythmia induced. This situation may result in hypotension but usually is short-lived and can be readily converted via intracardiac pacing. If hypotension is prolonged and intracardiac conversion is unsuccessful, transthoracic cardioversion may be necessary; therefore a defibrillator should be immediately available.
Congenital Heart Disease
Patients with pulmonary atresia and intact ventricular septum (PA/IVS) require careful examination of the coronary anatomy prior to decompressing the RV either surgically or with catheterization techniques, because of the possible presence of fistulas from the RV to the coronary artery circulation.18,19 RV to coronary artery fistulas can be seen on echocardiography, but selective right ventricular angiography and aortography, or even selective coronary angiography if necessary, are important to determine any associated coronary stenoses or atresia (RV-dependent coronary circulation).20 Myocardial ischemia can occur if the right ventricle pressure decreases after the outflow tract is opened, leading to arrhythmia and myocardial failure. At another end of this spectrum, patients with tetralogy of Fallot and pulmonary atresia often have diminutive native pulmonary arteries. Aortopulmonary collaterals may contribute greatly to pulmonary blood flow. Angiography can delineate the exact location and anatomy of these collaterals and, if indicated, may be followed by coil occlusion of aortopulmonary collaterals that provide dual supply to the native pulmonary arteries. It is important to know the extent of collateral vessels prior to surgery and cardiopulmonary bypass because of the risk for impaired systemic perfusion from excessive runoff to the pulmonary circulation.
Patients with hypoplastic left heart syndrome with mitral stenosis and aortic atresia (MS/AA) may also be at higher risk for early mortality after stage one palliation with the Norwood procedure.21 Analogous to the PA/IVS patient population, patients with MS/AA may have left ventricle-subepicardial coronary artery fistulae, and be at risk for inadequate myocardial protection during cardiopulmonary bypass and ischemia following stage one palliation. Preoperative coronary angiography may be warranted in this subgroup prior to surgical palliation.22 Finally, preoperative angiography may be useful in patients with obstructed total anomalous pulmonary venous connection (TAPVC). While pulmonary venous anatomy can often be determined by noninvasive methods, palliative transcatheter approaches to relief of pulmonary venous obsruction may be lifesaving in the critically ill neonate.23,24
Therapeutic Interventions in the Newborn
Atrial Communication Procedures
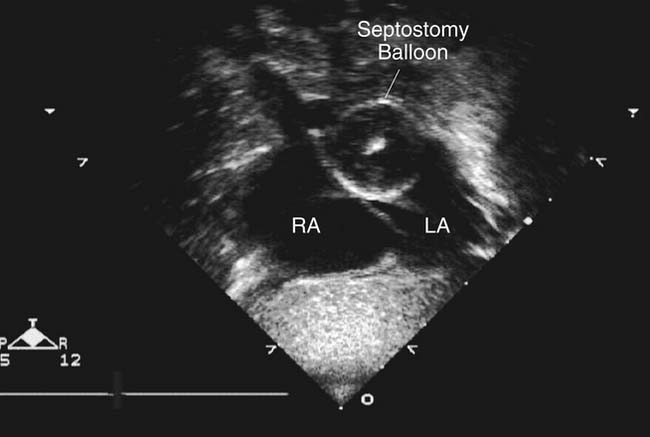
The first therapeutic procedure performed in the catheterization laboratory for congenital heart disease was balloon atrial septostomy (BAS) in newborns diagnosed with transposition of the great arteries (TGA) with intact ventricular septum.25 A BAS usually is needed in newborns with TGA to facilitate mixing of systemic and pulmonary venous return at the atrial level prior to the arterial switch operation. This procedure can be performed by echocardiographic guidance26 (Figure 24-1) or in the cardiac catheterization laboratory if additional diagnostic information is required or there are potential vascular access problems. Via either the femoral or umbilical vein, a balloon catheter is advanced across the atrial defect from right atrium to left atrium (Figure 24-2, A) and its position is confirmed by echocardiographic or fluoroscopic guidance. The balloon is inflated to the desired volume and jerked back to the right atrium to tear the septum primum (Figure 24-2, B). While it has been reported that BAS may be associated with an increased risk for embolic neurological injury, this has not been the experience at our institution and others. It is always preferable to facilitate mixing at the atrial level and reduce left atrial pressure and risk for pulmonary hypertension prior to cardiac surgery and the arterial switch procedure. The BAS can be performed under fluoroscopic or echocardiographic guidance, and whatever the mode of imaging, it is important that anticoagulation with 50 U/kg of heparin be administered prior to balloon inflation and tearing of the atrial septum.27–29
< div class='tao-gold-member'>





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


