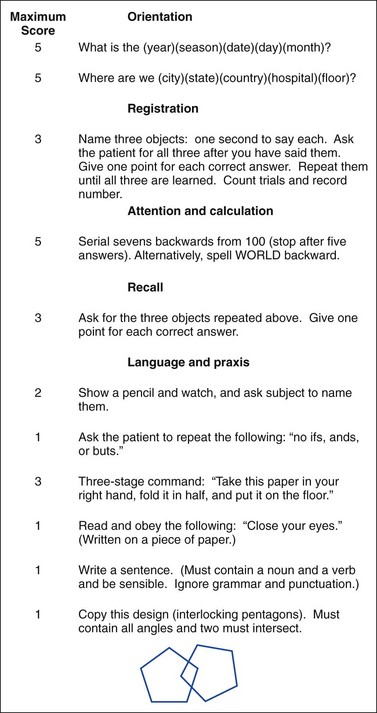
Chapter 104 In the past, terms such as acute confusional state, sundowning, and organic brain syndrome have been used to describe a host of abnormal cognitive states that can be observed in the emergency setting. These terms have loosely defined a group of neurobehavioral disorders that are caused by a physiologic disturbance. Organic brain syndrome is a nebulous term that the Diagnostic and Statistical Manual of Mental Disorders (fourth edition, text revision) eschews because the “organic” connotation implies that so-called functional mental disorders are without a biologic basis.1 1. The first step is to determine whether this state represents delirium or dementia. The clinical findings may be subtle, and establishment of the diagnosis can be challenging, especially because delirium may be superimposed on dementia and dementia remains an independent risk factor for delirium.2,3 Early symptoms and signs may go unrecognized unless an adequate history is obtained from the patient, family members, and caregivers. A careful examination must include memory and cognitive assessment with a mental status screening examination. 2. Supportive care must be provided. This care may range in extent from aggressive airway and cardiovascular support to pharmacologic or physical restraint to simply placing the patient in a quiet room with appropriate environmental support. 3. A diligent search must be initiated for the underlying precipitating stressors in patients presenting with delirium. Several key features are necessary for a diagnosis of delirium (Box 104-1). Patients with delirium have disturbances in consciousness, memory, cognition, and perception. These disturbances tend to develop during a short time (hours to days). The disturbance in consciousness may be manifested initially as an inability to focus attention. The fluctuating course of symptoms and inattention are the hallmarks of delirium. Deficiencies in cognition may be manifested by disorientation and memory deficits. Perceptual disturbances include hallucinations and delusions. The delirious patient may be somnolent or agitated, and the thought process may range from mildly disturbed to grossly disorganized. The clinical presentation may be subdued or explosive. The patient’s sleep-wake cycle may be altered or reversed; agitation often is present during the night. Historically, delirium referred to a hyperactive state marked by agitation and emotional lability (e.g., delirium tremens). An important point, however, is that delirium has several psychomotor subtypes: hyperactive (mania), hypoactive (depressed), and mixed type.4 The exact incidence of delirium in the overall ED population is unknown. However, the prevalence of delirium among elders who present to the ED is approximately 10 to 20%.5 Geriatric patients are at particularly high risk for the development of delirium. Advanced age, dementia, and underlying medical illness are strongly associated with delirium. Multiple medications, drugs, and alcohol also are associated with delirium.6 Severe psychological stress and sleep deprivation may facilitate the development of delirium. Although the exact pathophysiologic process is not well understood, multiple neurotransmitters have been implicated in causing delirium. One theory is that delirium is associated with a derangement of central cholinergic transmission. Serum anticholinergic activity is increased, and low levels of acetylcholine are seen in older patients with delirium.7 Increased serotonin levels have been found in hepatic encephalopathy, serotonin syndrome, sepsis, and psychedelic drug ingestion.8 Some of the disturbances that occur in delirium are deficiencies of substrates for oxidative metabolism (e.g., glucose, oxygen); disturbances of ionic passage through excitable membranes; increase in cytokines; imbalance of normal noradrenergic, serotoninergic, dopaminergic, and cholinergic homeostasis; and, in some cases, synthesis of false neurotransmitters.9 Drugs and exogenous toxins can produce delirium through direct effects on the CNS. Although the limbic system appears to be particularly vulnerable to the effects of these drugs, the cerebral hemispheres and the brainstem also can be profoundly affected. The causes of delirium are legion (Table 104-1). Within the geriatric population, medications are a common cause of delirium, whereas drugs (including ethanol) are the most common cause of delirium in the younger adult population. Acute cognitive dysfunction may be secondary to drug overdose, withdrawal syndromes, and adverse or idiosyncratic reactions. Table 104-1 Causes of Delirium: “I Watch Death” Mnemonic Modified from Wise MG: Delirium: Differential diagnosis for delirium: Critical items (I WATCH DEATH). In: Yudofsky SC, Hales RE (eds): The American Psychiatric Press Textbook of Neuropsychiatry, 2nd ed. Washington, DC, American Psychiatric Publishing, 1992. The list of commonly prescribed drugs causing delirium is extensive and includes antibiotics (antifungal, antimalarial, and antiviral agents; numerous antibacterial agents, including the quinolones and macrolides), anticholinergic drugs (antihistamines, antispasmodics, muscle relaxants, tricyclic antidepressants), anticonvulsants, anti-inflammatory agents (corticosteroids, salicylates, and other nonsteroidal anti-inflammatory drugs), various cardiovascular medications (beta-blockers, antidysrhythmics, antihypertensives, cardiac glycosides), sympathomimetics (phenylpropanolamine), sedative-hypnotics, narcotics (transdermal fentanyl [Duragesic], morphine sulfate [Roxanol], hydromorphone HCl [Dilaudid], oxycodone HCl [OxyContin]), miscellaneous drugs (aminophylline, cimetidine, lithium, chlorpropamide), over-the-counter medications with anticholinergic properties, and caffeine-containing products.6 Acute confusional states have been reported to be a more common herald of the onset of physical illness in the elderly than are fever, pain, and tachycardia.2,3,10 Factors that predispose elders to delirium include the effects of aging on the brain, reduced capacity for homeostatic regulation, impaired vision and hearing, and age-related changes in the pharmacokinetics and pharmacodynamics of drugs.11 The etiology of delirium in elders is usually multifactorial. The clinical manifestations of delirium are as variable as the causes. The clinical presentation can be so subtle as to go unrecognized or may be dramatic enough to disrupt the entire ED. The natural history of a patient’s delirium can progress from apathy to marked agitation in the course of hours (see Box 104-1). Nonspecific prodromal symptoms such as anxiety, restlessness, and insomnia typically emerge during hours to days. The physical examination is not often helpful in determining the specific drug or class of drugs causing acute cognitive impairment. The one exception to this rule is toxidromes, which are constellations of signs and symptoms characteristic of intoxication with certain drugs or classes of drugs (see Chapter 147). A brief mental status examination should be performed in all patients thought to have acute brain dysfunction. Although the concept is rather obvious, few physicians proceed beyond questions about the patient’s orientation to person, place, and time when assessing mental status. Failure to diagnose subtle forms of delirium when they are present is directly related to omission of mental status testing.12 Several standardized tools for assessment of mental status have been successfully applied in the ED.12–14 Mental status testing includes assessment of orientation, memory, attention, and concentration; several tests also incorporate assessments of constructional tasks, spatial discrimination, arithmetic ability, and writing. Cognitive functioning can be rapidly assessed in approximately 7 to 10 minutes. Memory assessment requires testing of the patient’s ability to repeat short series of words or numbers (immediate recall), to learn new information (short-term memory), and to retrieve previously stored information (long-term memory). Constructional apraxia is assessed by having the patient perform tasks such as drawing interlocking geometric figures or clock faces and connecting dots. Dysnomia (inability to name objects correctly) and dysgraphia (impaired writing ability) are two of the most sensitive indicators of delirium. Almost all acutely confused patients exhibit writing impairments, including spatial disorganization, misspelling, and tremor.13,15 No single bedside cognitive test that can be administered quickly is ideal. The Mini-Mental State Examination (MMSE) developed by Folstein and colleagues has been validated more than any other test and most frequently is recommended as a rapid screening tool.10,13,15,16 For hospitalized patients, this test has a sensitivity of 87% and a specificity of 82% for detection of organic brain syndrome. Some investigators report slightly better results when the test is modified and age is added as a variable in the analysis.16 The MMSE does not measure executive function and is insensitive for detection of early signs of mild cognitive impairment (without dementia) or early dementia.17 The MMSE consists of a short series of questions that test orientation, registration (memory), attention, calculation, recall, and language (Fig. 104-1). The time for the test to be administered can be reduced to 5 minutes by elimination of the writing and drawing components with only a modest reduction in sensitivity. The registration section tests both immediate and short-term memory; the recall section also assesses short-term memory. The ability to recall two of three objects has 81% sensitivity and 74% specificity for exclusion of organic brain syndrome. Asking the patient to subtract “serial sevens” backward from 100 assesses attention, concentration, and arithmetic ability. This test is specific but not sensitive for absence of an organic brain syndrome; up to 40% of nondelirious, nondemented people fail to perform the tasks of this test correctly, reflecting limitations due to language ability and education. A total score of 23 or less is considered markedly abnormal and indicates an organic brain syndrome. As a general rule, patients with mild cognitive impairment have a score of 18 to 26 of 30, those with moderate impairment have a score of 10 to 18, and those with severe impairment have a score of less than 10. The Quick Confusion Scale represents another attempt to quantify the attention aspects of mental status (see Chapter 17, Fig. 17-2). It has significant correlation with the MMSE, can be administered more quickly, and does not require constructional tasks.18 Another useful diagnostic tool is the Confusion Assessment Method; it has a sensitivity of 93 to 100% and specificity of 90 to 95%.19 This simple tool has four key features used for screening of delirium: acute onset and fluctuating course, inattention, disorganized thinking, and altered level of consciousness. For a definitive diagnosis of delirium, the first two features and one of the last two must be present. It has proved to be a valuable tool because of its ease and interobserver reliability. In addition, it has been shown to be more sensitive than clinical impression alone.18,20 The Six-Item Screener is another brief test of cognition that was found to be 94% sensitive and 86% specific in identifying disturbance of cognition in older patients.15 Some reversible causes of delirium can be diagnosed by a number of basic, readily available tests. The following laboratory tests can be helpful in evaluation of the delirious patient: a complete blood count (CBC; hemoglobin, leukocyte count with differential, platelet count, and mean corpuscle volume), serum electrolyte values, glucose concentration, calcium concentration, and urinalysis. The CBC may suggest unusual but potentially treatable abnormalities, such as thrombotic thrombocytopenic purpura, megaloblastic anemia, hyperviscosity from myelogenous leukemia, and unsuspected infection. The anion gap should be determined in all patients with altered mental status. An elevated anion gap (>15 mEq/L) may indicate the presence of unmeasured anions, such as sulfate in renal failure; keto acids in diabetic or alcoholic ketoacidosis; lactate in postictal states or associated with hypotension; and exogenous toxins, such as ethylene glycol, methanol, and salicylates. A pulse oximetry measurement should be obtained in all patients to screen for hypoxemia, and an arterial blood gas analysis is warranted in those patients at risk for respiratory failure with carbon dioxide retention. Suspected occult infection warrants urinalysis and chest radiography. In elders, an electrocardiogram should be obtained to exclude a silent acute coronary syndrome. Ammonia level should be considered in patients with cirrhosis, ascites, or asterixis. Despite these diagnostic evaluations, no cause is found for delirium in up to 16% of patients.6 Considerations in the differential diagnosis for apparent delirium include functional psychiatric disorders and dementia. Depression, mania, paranoia, and schizophrenia all may resemble delirium. Several clinical features are helpful in distinguishing between organic and functional syndromes (Table 104-2). Table 104-2 Comparison of Delirium and Acute Psychosis
Delirium and Dementia
Perspective
Delirium
Pathophysiology
Etiology
CAUSE
FORM
Infectious
Sepsis, encephalitis, meningitis, syphilis, central nervous system abscess
Withdrawal
Alcohol, barbiturates, sedative-hypnotics
Acute metabolic
Acidosis, electrolyte disturbance, hepatic or renal failure, other metabolic disturbances (↑ or ↓ glucose, magnesium, calcium)
Trauma
Head trauma, burns
CNS disease
Hemorrhage, stroke, vasculitis, seizures, tumor
Hypoxia
Acute hypoxia, chronic lung disease, hypotension
Deficiencies
Vitamin B12, hypovitaminosis, niacin, thiamine
Environmental
Hypothermia, hyperthermia, endocrinopathies (diabetes, adrenal, thyroid)
Acute vascular
Hypertensive emergency, subarachnoid hemorrhage, sagittal vein thrombosis
Toxins or drugs
Medications, street drugs, alcohol, pesticides, industrial poisons (e.g., carbon monoxide, cyanide, solvents)
Heavy metals
Lead, mercury
Clinical Features
Diagnostic Evaluation and Ancillary Studies
Differential Diagnosis
CHARACTERISTIC
DELIRIUM
ACUTE PSYCHOSIS
Onset
Acute
Acute
Vital signs
Typically abnormal (fever, tachycardia)
Normal
Prior psychiatric history
Uncommon
Common
Course
Rapid, fluctuating
Stable
Psychomotor activity
Variable
Variable
Involuntary activity
Possible asterixis, tremor
Absent
Cognition function
Orientation
Usually impaired
Occasionally impaired
Attention
Globally impaired
May be disorganized
Concentration
Globally impaired
Impaired
Hallucinations
Visual, visual and auditory
Primarily auditory
Delusions
Transient, poorly organized
Systematized
Speech
Pressured, slow, possibly incoherent
Usually coherent
Course
Typically resolves
Responds to therapy, recurrence common ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Delirium and Dementia
Only gold members can continue reading. Log In or Register to continue



