47 Complications of Bariatric Surgery
 Key Points
Key Points• Laparoscopic Roux-en-Y gastric bypass is the most commonly performed bariatric procedure in the United States.
• Pulmonary embolism (30% to 40%) is the most common cause of death after bariatric surgery, followed by cardiac events (25%) and anastomotic leaks (20%). Dumping syndrome, wound infections, strictures, and stomal ulcerations are common complications.
• Acute gastric distention is a rare but potentially deadly early postoperative complication that requires decompression.
• A nasogastric tube could perforate the pouch site in patients who have recently undergone surgery.
• Abdominal pain without vomiting in the early postoperative weeks might represent a small bowel obstruction or internal hernia.
• Laparoscopic adjustable gastric banding (LAGB) is the most commonly performed bariatric procedure in Europe and is becoming more common in the United States.
• Acute anterior or posterior gastric band slippage is the most common complication of LAGB requiring emergency treatment (band deflation).
• LAGB has the lowest morbidity and mortality of all currently performed bariatric procedures.
Epidemiology
The prevalence of morbid obesity has risen more than fourfold since 1986.1 Currently, 1.7 billion people worldwide are considered obese and approximately 60% of the U.S. population is overweight. In excess of 100 billion dollars is spent annually on obesity health care–related costs.
To be considered morbidly obese, one must have either a body mass index (BMI) greater than 40 kg/m2 or a BMI of 35 to 40 kg/m2 with comorbid conditions.2 More than 15 million Americans currently have BMI levels that make them eligible for bariatric surgery.3 In the United States only about 1% of eligible patients undergo bariatric surgery.
Morbid obesity promotes the development of diabetes mellitus, hypertension, dyslipidemia, cardiovascular disease, gastroesophageal reflux, asthma, and obstructive sleep apnea. Premature death from obesity now rivals the mortality rates related to smoking, with more than 300,000 deaths attributable to obesity per year.4
Bariatric surgery is the most effective and durable treatment to achieve weight loss and its associated comorbidity. Five-year mortality is reduced 89% in severely obese patients who undergo weight loss surgery.5,6 Fifteen-year survival increases by one third in patients who undergo bariatric surgery in comparison with those who do not. New laparoscopic surgical techniques have contributed to the growing demand for and acceptance of bariatric surgery. Approximately 4925 bariatric procedures were performed in 1990, as compared with an estimated 220,000 in 2008. Bariatric surgery is now the second most common abdominal operation in the United States.
Recent trends suggest that higher-risk, older patients are undergoing bariatric procedures with greater frequency; surprisingly, they demonstrate postoperative morbidity and mortality rates similar to those in the general population.7 Rates of perioperative complications, reoperation, hospital readmission, and emergency department (ED) visits have been falling. The rates for these indicators are highest with gastric bypass followed by sleeve gastrectomy and lowest for laparoscopic adjustable gastric banding (LAGB).8 Overall, in-hospital mortality rates are between 0.05% and 0.2%, and 30-day mortality rates have been reported to range between 0.05% and 2%.
Complications of bariatric surgery are common and are generally initially treated in the ED. Up to 20% of patients are admitted for a postoperative complication within 1 year of the bariatric procedure; this rate increases to 40% within 3 years. The potential postoperative complications of the various bariatric procedures have predictable timing and clinical manifestations.9
Types of Bariatric Surgery: Roux-en-Y and Gastric Banding
The two most common types of bariatric surgery in the United States are the Roux-en-Y gastric bypass (RYGBP) (54%) and adjustable gastric banding (39%). Adjustable gastric banding continues to rapidly gain in popularity since initial federal approval in 2001.7
Malabsorption
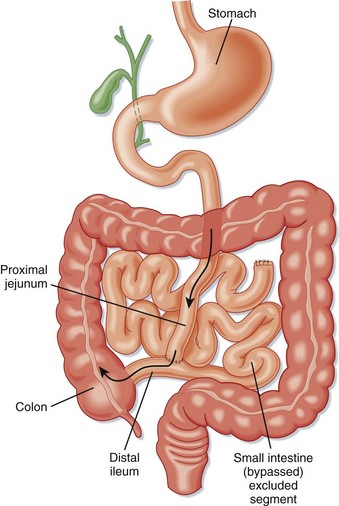
Surgical techniques that induce malabsorption were the first attempted. Malabsorptive techniques were thought to be the most effective method of achieving rapid and sustained weight loss. Surgeons initially connected the proximal jejunum to a distal portion of the ileum or ascending colon in a procedure known as jejunoileal bypass (Fig. 47.1). This technique resulted in severe diarrhea, dangerous metabolic derangements, arthropathy, renal calculi, gallstones, liver disease, and short bowel syndrome. Gastric bypass has been shown to be a more effective malabsorptive procedure with fewer side effects than those associated with jejunoileal bypass. Malabsorptive procedures still in current use include laparoscopic RYGBP, BPD, duodenal switch, and isolated intestinal bypass.
Restriction
Purely restrictive procedures are less effective than malabsorptive techniques.6 Restrictive surgeries act by reducing oral intake through induction of early satiety. However, some areas of the stomach easily dilate over time, which causes gradual increases in perceived hunger and subsequent food intake. Restrictive procedures are more successful when the lesser-curve gastric pouch is 15 mL or smaller.4 Restrictive weight loss procedures such as vertical banded gastroplasty and isolated partial gastrectomy (sleeve gastrectomy) have fallen out of favor. LAGB is the most common, poses the least risk, and is the most effective restrictive technique currently performed.10
Roux-en-Y Gastric Bypass
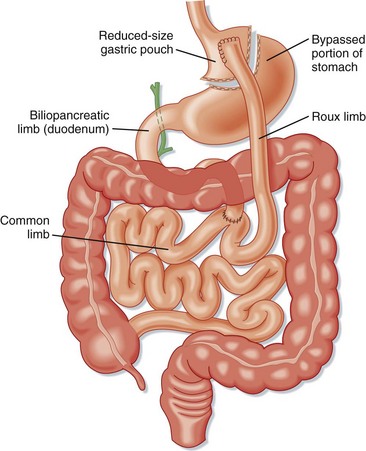
The RYGBP procedure creates a gastric pouch from the proximal portion of the lesser curvature of the stomach that can hold about 15 to 30 mL of fluid and food (Fig. 47.2). A portion of the distal end of the small bowel is connected to this pouch to create a concurrent malabsorptive process. Historically, RYGBP was an open procedure, but currently the majority are performed laparoscopically.
Late complications generally involve both anatomic and systemic complications. Anatomic complications include esophageal reflux, chronic abdominal pain, internal hernias, ulcers, stricture, stenosis, and bowel obstruction. Systemic complications are manifested mostly as nutritional deficiencies.11 Clinical manifestations include anemia (iron deficiency), osteopenic fractures (calcium deficiency), fatigue and lower extremity edema (protein-calorie malnutrition), chronic pain and proximal muscle weakness (vitamin D deficiency), visual deficits (vitamin A deficiency), and vague neurologic symptoms (thiamine, folate, and vitamin B12 deficiencies).
Specific Clinical Presentations
The occurrence of acute fever and tachycardia within weeks of a Roux-en-Y procedure suggests an anastomotic leak with or without abscess formation. The symptoms are often subtle but can include dyspnea, unexplained sepsis, changes in mental status, and restlessness. Peritoneal signs are often lacking. Because abdominal examination of morbidly obese patients is unreliable, the diagnosis is best accomplished through imaging studies. CT of the abdomen and pelvis with oral and intravenous (IV) administration of a contrast agent is the modality of choice. If the patient is unable to undergo CT because of the weight limitations of the CT table, an upper GI radiographic series should be obtained. The false-negative rate is high (up to 44%) with CT and other imaging studies for the evaluation of anastomotic leaks. Laparoscopy should be considered in cases of negative imaging but high pretest probability of an anastomotic leak.12,13




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


