146 Clostridium difficile Colitis
Antibiotic-associated colitis was recognized soon after antibiotics were introduced in the 1940s, but the cause was not known until 1978 with the original reports of the role of Clostridium difficile as the putative agent in nearly all cases of antibiotic-associated pseudomembranous colitis and 10% to 15% of those with uncomplicated antibiotic-associated diarrhea.1 Subsequent work has identified the pathophysiology, epidemiology, diagnostic methods, and treatment for this condition. The major challenges continue to be prevention and the management of patients with advanced disease, particularly those with ileus.
 Etiology
Etiology
C. difficile causes a spectrum of enteric complications of antibiotic use ranging from nuisance diarrhea to severe and sometimes life-threatening pseudomembranous colitis. There are occasional cases of antibiotic-associated colitis due to other pathogens (Staphylococcus aureus, Klebsiella oxytoca, enterotoxin-producing strains of Clostridium perfringens or Salmonella), but most cases are either due to C. difficile or are enigmatic.2
 Pathophysiology
Pathophysiology
There are six relevant issues:
 Clinical Signs and Symptoms
Clinical Signs and Symptoms
The typical presentation of Clostridium difficile infection (CDI) is watery diarrhea associated with cramps.2 Other common features are fecal leukocytes, endoscopy showing PMC or colitis, characteristic changes on computed tomography (CT) (thickened bowel restricted to the colon, often associated with ascites), fever, hypoalbuminemia, and leukocytosis, sometimes with a leukemoid reaction. Nearly all cases of CDI are associated with diarrhea, but occasional postoperative patients will not have this owing to ileus. The laboratory clue that best predicts this diagnosis and its severity is the white blood cell (WBC) count. The average is about 15,000 cells/mL, but it may be much higher with counts over 20,000 or even 50,000 cells/mL. This strongly supports the CDI diagnosis and predicts severe disease.8
 Diagnosis
Diagnosis
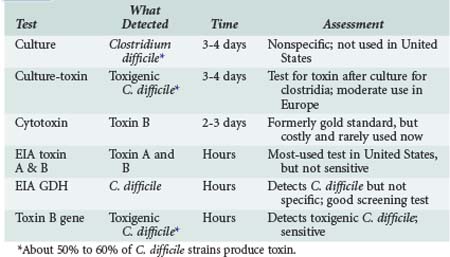
The diagnosis is based on detection of the C. difficile (culture, EIA for glutamine dehydrogenase or polymerase chain reaction [PCR] for toxigenic C. difficile) or its toxins, designated toxin A and toxin B (enzyme immunoassay [EIA] for toxins A + B, or cytotoxin assay). Relative merits are shown in Table 146-1.
 Treatment
Treatment
Most important to treatment of CDI is discontinuing the implicated antibiotic. If there is a need for antibiotic treatment, select a drug that is unlikely to cause CDI (narrow-spectrum β-lactams, macrolides, aminoglycosides, antistaphylococcal drugs, tetracyclines; Table 146-2). The two favored drugs for treatment of CDI are metronidazole and vancomycin, both given by mouth.1,6,7 Metronidazole is often preferred because it is less expensive. Earlier studies showed it to work as well as vancomycin, but more recent trials show oral vancomycin is superior to metronidazole in seriously ill patients,8 defined as having a WBC over 15,000 cells/mL or elevated creatinine to 1.5 × baseline.6 Other markers of serious disease are albumin less than 2 mg/dL, admission to the ICU for CDI, pseudomembranous colitis (PMC) on endoscopy, or pancolitis on CT scan.9 Vancomycin is superior to metronidazole owing to pharmacology.8 All C. difficile are in the colon, so the challenge is getting an active drug to the colonic lumen. Vancomycin is not absorbed, so it all goes to the colon when given orally; metronidazole given orally is nearly completely absorbed, so it gets to the colon primarily through an inflamed colonic mucosa. Most patients improve with resolution of diarrhea in 3 to 5 days.1,7 Patients who are seriously ill (megacolon, septic shock, WBC >30,000/mL, lactate >5) and fail to respond to standard treatment should be considered for colectomy.9 The major indications are failure to respond to standard medical management and colonic perforation.
TABLE 146-2 Treatment of Clostridium difficile Infection
| Category | Characteristics | Treatment Recommendations |
|---|---|---|
| Mild-moderate | WBC ≤ 15,000/mL and creatinine < 1.5 × baseline | Metronidazole 500 mg PO 3×/d × 10-14 days |
| Severe | WBC > 15,000/mL or creatinine > 1.5 × baseline | Vancomycin, 125 mg 4×/d PO × 10-12 days |
| Severe and complicated | Hypotension, shock, ileus or megacolon | Vancomycin, 500 mg PO 4×/d by NG tube or by rectum, plus Metronidazole 500 mg IV q 8 h |
| First relapse Second relapse | As above Vancomycin, standard dose, then taper and/or pulse |
PO, per os (orally); NG, nasogastric; WBC, white blood cell.
Adapted from Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol 2010;31:431-55.





