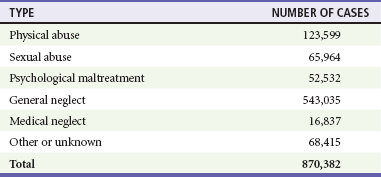
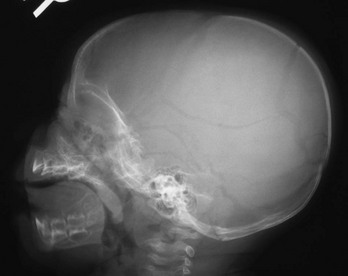
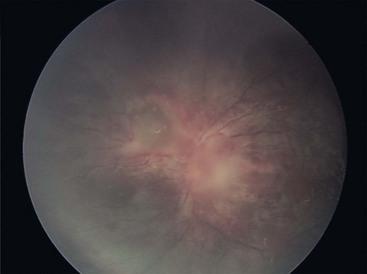
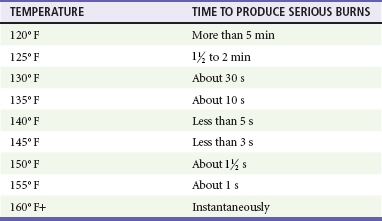
Chapter 66 Child maltreatment is an all-encompassing term that includes all forms of child abuse: physical abuse, sexual abuse, emotional abuse, child neglect (physical, emotional, educational), and factitious disease by proxy (also known as Munchausen syndrome by proxy and most recently termed medical child abuse).1,2 Although the recognition of these conditions by the medical community has occurred at different times, the pivotal report describing child physical abuse, published in 1962, was the article “The Battered Child Syndrome” by Kempe and colleagues.3 The article noted the presence of a complex of physical findings, including fractures, cutaneous bruises, and internal injuries. Since that time, multiple articles and books have described the spectrum of the disorders. During the 1980s, much of the literature focused on child sexual abuse, including the refinement of understanding of normal anogenital anatomy of prepubescent children.4 Child sexual abuse is defined as the involvement of children and adolescents in sexual activity to which they cannot give consent based on their developmental level, involving an age disparity between the victim and the perpetrator, and for the sexual gratification of the older individual. Child sexual abuse may involve physical contact between the child and the adult or the involvement of the child in other activities, such as photography or the production of pornographic material. Just under 1 million cases of suspected child abuse and neglect are reported annually in the United States. Table 66-1 summarizes the data by category of abuse or neglect as noted by the 2009 Child Maltreatment report from the U.S. Department of Health and Human Services.5 Although child abuse occurs across the spectrum of race, ethnicity, and socioeconomic class, certain factors are associated with an increased prevalence of abuse, including poverty, social isolation, parental alcohol and substance abuse, parental mental illness, and domestic violence.6,7 Table 66-1 Overview of Incidence of Child Abuse Data from U.S. Department of Health and Human Services, Administration on Children, Youth and Families: Child Maltreatment 2009. Washington, DC: U.S. Government Printing Office; 2010. Available at http://www.acf.hhs.gov/programs/cb/stats_research/index.htm#can. Accessed January 11, 2013. Bruises may appear as petechiae or ecchymoses. They occur at the point of impact between the striking object, such as the hand, and the child’s body. Often they mirror the form of the inflicting object and may appear as a hand print, a belt outline, or a mark resembling another object (Fig. 66-1). These bruises are referred to as patterned injuries. When the blow occurs at high velocity, the bruising may resemble the outline of the object as the soft tissue in the center of the impacted field moves laterally (negative image). When the thrust of the strike is slower, the central portion of the skin also may be discolored (positive image). The extent of an injury is influenced by many factors, including the force of blow and the area struck. Frequently, the struck area initially is only erythematous, swollen, or tender, and 24 hours may elapse before bleeding into the skin and subsequent discoloration are noted. The degree of discoloration and the rapidity of resolution of the discoloration are influenced by the location of the injury; large fat pads or muscle masses, such as the buttocks, can hold larger volumes of blood, and resolution takes longer. In general, extravasated blood goes through a predictable color change pattern as it resolves, progressing from purple to green to yellow and eventually to brown. However, the color of a bruise should not be used as a tool to estimate the age of a bruise.8,9 Accidentally incurred bruises tend to occur over bony prominences, such as the shin and forehead. In addition, nonambulatory children (<1 year old) do not readily sustain accidental cutaneous injuries (“those who don’t cruise, don’t bruise”).8 Bites also produce a patterned injury. The distance between the maxillary canine teeth helps establish whether the perpetrator was a child (<2.5 cm), which is often alleged, or an adult (>3 cm) (Fig. 66-2).10 Burns may be inflicted through contact with a dry hot object or through immersion in hot water. One common type of inflicted burn occurs secondary to contact with a cigarette. Inadvertent contact with a lit cigarette tends to create less severe or linear burns; however, inflicted cigarette burns are usually circular, measuring 8 to 10 mm (Fig. 66-3). Initially they have a blistered appearance but then become ulcerated and crust over. Burn injuries also may assume a patterned appearance resembling the configuration of the hot object, such as a heating grid or an iron. Immersion burns occur when a child or infant is placed in hot water. Such burns often involve the anogenital area and may represent punishment for toilet training accidents, or they involve hands or feet (glove-stocking distribution) that have been dunked in hot water. Immersion burns are usually second-degree burns (Fig. 66-4). The extent of the burn is influenced by the temperature of the water, the body site exposed (the skin is thinner in certain areas, such as the anogenital region), the age of the individual (younger children and elderly adults have thinner skin), and the duration of the contact between the hot object and the skin (Table 66-2).11 Burns caused by contact with viscous liquids, such as grease, oils, or syrups, may be more severe because such liquids are more adherent to the skin surface. Chemical burns may occur through contact with corrosive products, including industrial-strength cleaning agents. Accidental burns can occur in children and usually involve scald injuries, which happen when children spill hot liquids, such as coffee, on their clothes and skin. Spill burns have a characteristic drip appearance, with more extensive and severe injury proximal to the point of contact and less extensive and milder injury more distally (Fig. 66-5). Disposable diapers are very absorbent of heat as well as of liquids. Scald burns in the anogenital area that are attributed to hot beverages falling into a child’s diaper should be scrutinized carefully, and if there is any concern of abuse, a report should be made by anyone who is considered a mandated reporter such as a paramedic, nurse, physician, or social worker.12,13 The report is made to child protective services or law enforcement. Many jurisdictions have a “child abuse hotline” to facilitate such reporting. Skeletal injuries may involve any of the bones in the body. Although approximately 42% of boys and 27% of girls have sustained a fracture before the age of 16 years, certain fractures are highly suspicious of an inflicted injury (Table 66-3).14,15 In particular, metaphyseal fractures, rib fractures, and certain types of skull fractures should raise concern about inflicted trauma (Fig. 66-6). Metaphyseal fractures (i.e., classic metaphyseal lesions) occur because of yanking or pulling on an extremity. On radiographs they may appear as metaphyseal chips or what is referred to as a bucket-handle injury of the metaphysis of the long bone. They are characterized by the absence of callus as they heal (Fig. 66-7). They usually are noted in children younger than 2 years. Long bone fractures involving the lower extremities are equally concerning in preambulatory children. Once children are ambulatory, accidental injuries such as toddler factures (nondisplaced spiral fractures of the distal tibia) are not uncommon. Rib fractures, particularly posterior rib fractures in an otherwise healthy infant, are virtually pathognomonic for inflicted injury16 (Fig. 66-8). The rib cage, because of its archlike structure, must be subjected to a good deal of force for disruption to be caused. Rib fractures are extremely uncommon as a consequence of cardiopulmonary resuscitation (CPR) and are not reported across the age spectrum. In addition, there is no evidence that chest encirclement for CPR is more likely than two-finger sternal compression to cause rib fractures.17 The presence of multiple skull fractures or skull fractures in the occipital region is unusual in cases of accidental trauma and should raise concern for inflicted trauma. Fractures that are diastatic (>3 mm in width) or grow in size are less specific as markers for nonaccidental trauma; however, they are usually associated with mechanisms of injury that involve greater traumatic forces. Table 66-3 Figure 66-6 Complex skull fracture associated with child maltreatment. (Courtesy Sara T. Stewart, MD, MPH.) Head injuries, including those associated with the classically described “shaken baby syndrome,” account for most child abuse–related fatalities. The syndrome includes evidence of head trauma in association with retinal hemorrhages and skeletal injuries and occurs generally in infants younger than 1 year but may be seen in children up to 3 years old. Often, there is no evidence of an impact injury to the head, such as a scalp hematoma or skull fracture.18,19 If impact occurs, it may be against a soft or compressible surface, such as the mattress of the crib. Such an impact results in a rapid deceleration of the head, and the brain experiences a coup-contrecoup injury by moving back and forth within the confines of the skull. Some infants have been subjected to multiple episodes of shaking.20 Shaking of an infant or young child subjects the brain to rotational acceleration, which is capable of generating greater force and speed than linear acceleration, which is the type of acceleration that occurs with a fall. It has been postulated that severe repeated shaking of an infant or young child can lead to disruption of the neuronal cells, with or without the presence of either subarachnoid or subdural hemorrhage. Hemorrhage is a marker for the event but may be of limited clinical significance, and death, when it occurs, may not be related to bleeding, brain compression, or brain displacement. Injury to the brain cells is referred to as traumatic axonal injury. This injury results in disruption of the cell membrane and subsequent cerebral edema. Cerebral edema impedes the cerebral circulation, which results in further hypoxic damage to the brain. At autopsy, special staining techniques allow for the recognition of axonal injury, which may be diffuse (diffuse axonal injury).21,22 Retinal hemorrhages are another common associated finding and are reported to be present in about 85% of cases of shaken baby syndrome. Approximately two thirds of these children have retinal hemorrhages that are multilayered, are too numerous to count, and extend to the periphery of the retina (Fig. 66-9). The pathophysiology of retinal hemorrhages is uncertain. Current evidence points to vitreoretinal traction as a significant factor in causing retinal hemorrhage as an infant’s head undergoes forceful rotational movement in which centrifugal forces are generated. It is unclear what role other factors, such as increased intracranial pressure and hypoxia, may have on the development of these hemorrhages as well. Hemorrhages may involve the vitreous in front of the retina, and retinal hemorrhages are categorized as preretinal, intraretinal, or subretinal. More superficial intraretinal hemorrhages that spread between nerve fibers may be described as flame or splinter hemorrhages, and deeper intraretinal hemorrhages may be described as “dot” or “blot” hemorrhages. Clinically, the hemorrhages may be localized or may extend to the ora serrata (the retinal edge). Extensive retinal hemorrhages have been shown to not result from typical resuscitation efforts but can occur from severe accidental mechanisms associated with rotational head movement, such as rollover motor vehicle collision or crush injuries to the chest with massive increase in intrathoracic venous pressure (Purtscher’s syndrome).23 Figure 66-9 Retinal hemorrhages in an infant with shaken infant syndrome. (Courtesy Carol Berkowitz, MD.) Abdominal trauma accounts for about 10% of injuries in abused children and carries a sixfold higher mortality rate than abdominal trauma caused by accidental means.24 Trauma is often blunt and includes blows and kicks to the abdomen. Frequently, there is no external evidence of the injury because the force has been transmitted to the intra-abdominal structures. Injuries that include hematomas or lacerations can occur to the liver or less commonly to the spleen. In addition, children may develop duodenal hematomas, an injury that leads to symptoms of upper intestinal obstruction. Perforations of the intestine or other hollow viscera can follow a blow to the abdomen, with subsequent progression to secondary peritonitis. Pancreatitis is also a sequela of inflicted abdominal trauma, which is said to be the most common mechanism of non–medication-associated pancreatitis in children. Pancreatic pseudocyst may develop as a complication of such trauma.25
Child Maltreatment
Perspective
Epidemiology
Principles of Disease
![]()
Stay updated, free articles. Join our Telegram channel












Full access? Get Clinical Tree


