202 Cardiovascular and Neurologic Oncologic Emergencies
 Key Points
Key Points• Early symptoms of cardiac tamponade are tachypnea and dyspnea with exertion.
• The superior vena cava (SVC) syndrome is caused by obstruction of blood flow through the SVC by compression or vascular thrombosis.
• Headaches from brain tumors are often described as tension-type headaches, but more frequently they have associated nausea and are sometimes worse with body positioning that increases intracranial pressure (i.e., leaning forward).
• In patients with spinal cord compression from malignant disease, pain may precede neurologic changes by several weeks. At the time of presentation to the emergency department, some motor weakness is usually evident.
• Corticosteroids and radiation therapy are typical initial treatments for spinal cord compression from malignant disease.
Cardiovascular Oncologic Emergencies
Cardiac Tamponade
Epidemiology
Malignant cardiac involvement is common, occurring in 11% to 12% of patients with cancer. Of these patients, three fourths have epicardial involvement, and one third of these patients have a pericardial effusion.1 The most common malignant primary tumor that progresses to involve the pericardium is lung cancer. Breast cancer, gastrointestinal cancers, melanoma, sarcoma, lymphoma, and leukemia account for most other cases. These tumors invade the pericardium through direct or metastatic spread. Less commonly, malignant primary pericardial tumors such as mesothelioma and sarcoma or benign tumors such as angioma, fibroma, or teratoma may occur. In a study conducted from 1996 to 2005, malignant disease was the primary cause of medical cardiac tamponade (65%), followed by unknown causes (10%), viral disease (10%), and anticoagulant medication–related intrapericardial bleeding (3%).2
Presenting Signs and Symptoms
Physical Findings
Patients with pericardial tamponade most commonly present with shortness of breath, hypotension, and often with clear lungs. Unfortunately, physical examination holds little value for diagnosing the presence of a pericardial effusion. However, as a malignant effusion becomes large enough to cause cardiac tamponade, some distinct physical findings may become evident. The Beck triad, first described in 1935, consists of increased jugular venous pressure, hypotension, and muffled heart sounds. However, this triad is most useful in acute cardiac tamponade, and it may be uncommon or difficult to assess in patients with atraumatic cardiac tamponade.3
Medical Decision Making and Diagnostic Testing
Electrocardiography
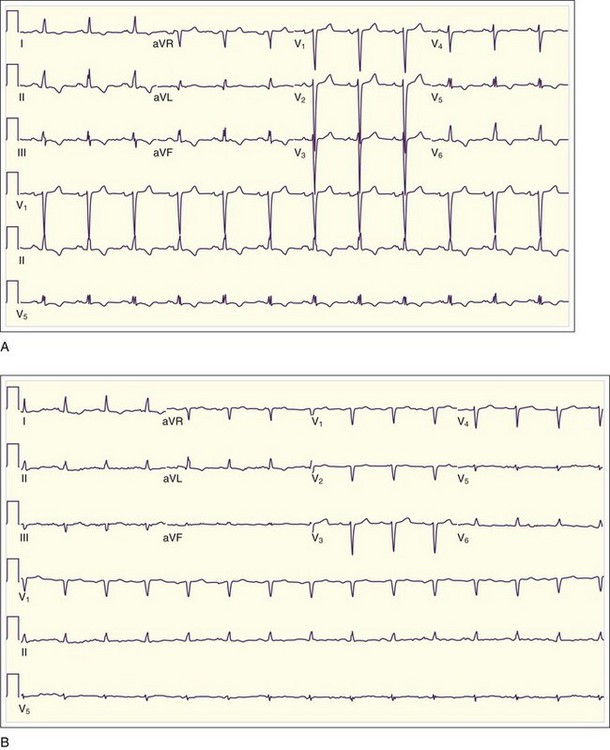
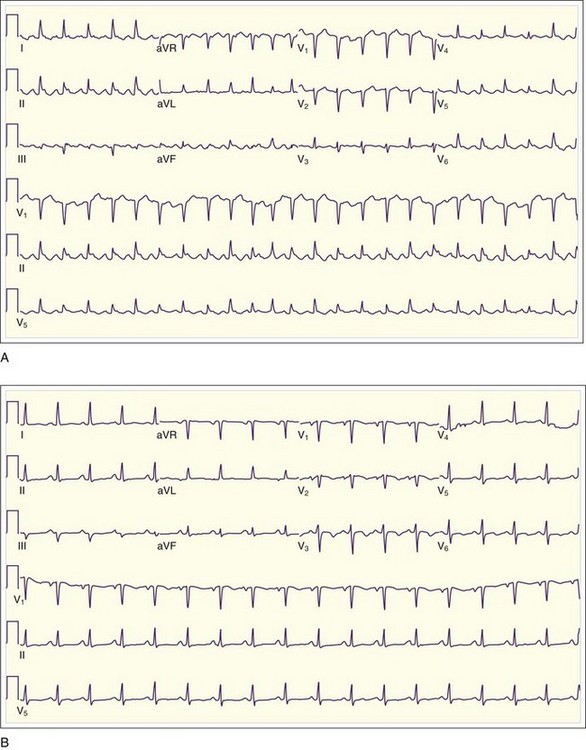
Low QRS voltage may be a sign of a large pericardial effusion, but it is more likely to be associated with tamponade physiology. In one small study, Bruch et al.4 studied 43 patients with a pericardial effusion. Of those patients, 14 of 23 with tamponade demonstrated low-voltage QRS complexes, as opposed to none of the 23 patients with effusion but without tamponade4 (Fig. 202.1). Electrical alternans (Fig. 202.2), demonstrated as beat-to-beat alterations in the amplitude of the QRS complex, is relatively specific but not very sensitive for cardiac tamponade. Electrical alternans may also rarely occur in patients with very large effusions without tamponade. Electrical alternans is caused by swinging of the heart in the pericardial effusion, and it generally disappears after removal of even modest amounts of pericardial fluid.
Chest Radiography
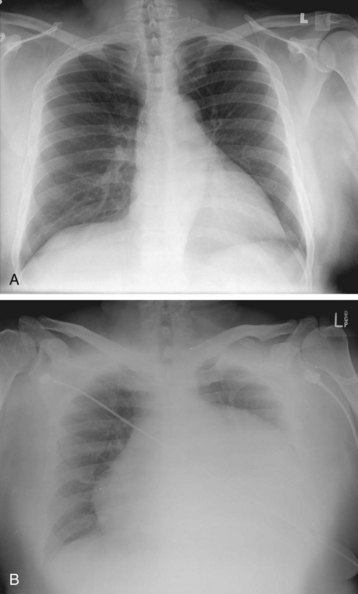
The typical finding on chest radiograph is an enlarged cardiac silhouette (the “water bottle”–shaped heart), as seen in Figure 202.3. In most cases, the lung fields are clear unless preexisting lung disease (e.g., malignant disease) is present. Cardiac tamponade may manifest without an enlarged cardiac silhouette if a small, rapidly accumulating effusion is the cause.
Echocardiography and Emergency Medicine Bedside Ultrasound
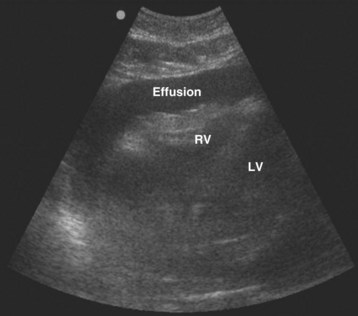
Echocardiography and emergency medicine bedside ultrasound play crucial roles in the diagnosis of cardiac tamponade. The first steps are to suspect a problem and to perform a screening cardiac ultrasound examination5 (Fig. 202.4).
Treatment
Pericardiocentesis may be performed under electrocardiographic or echocardiographic guidance. Echocardiographic guidance is preferred when available, because it allows greater precision of procedure direction and needle angle. Placement of an indwelling catheter is advisable, to prevent reaccumulation of fluid. The technique used for pericardiocentesis can be found in the “Tips and Tricks” box. Fluid obtained from pericardiocentesis should be sent for Gram stain, culture, acid-fast stain and culture, cytologic study, carcinoembryonic antigen determination, and polymerase chain reaction evaluation. Complications of pericardiocentesis are listed in Box 202.1.
Tips and Tricks
Technique for Pericardiocentesis Using Ultrasound Guidance
• Using bedside ultrasound, locate the ideal site of skin puncture where the largest fluid collection lies closest to the skin surface. This site is usually located on the left anterior chest wall. The clinician can choose either to mark the skin or to use the ultrasound device with a sterile sheath for dynamic guidance at this point.
• Prepare the skin in sterile fashion, and anesthetize the skin if time permits.
• Attach a 20-mL syringe to an 18-gauge spinal needle.
• Insert the needle at the site and trajectory determined by bedside ultrasonography. Take care to avoid the neurovascular bundle at the lower rib border and the internal mammary artery, which lies 3 to 5 cm lateral to the sternal border.
• Gently aspirate as the needle is advanced until fluid is obtained.
• Aspirate as much fluid as possible using the three-way stopcock.
• Alternately, use an over-the-needle catheter or the Seldinger technique if prolonged drainage is necessary. The Seldinger technique is performed using the same methods as outlined, but the clinician may use a thin-walled 18-gauge needle to pass a guidewire, followed by a catheter (e.g., a pigtail catheter) that may be left in place.
Disposition and Prognosis
Patients with cardiac tamponade are admitted to the hospital, typically in a cardiac care or intensive care unit (see the “Priority Actions” box). Emergency referral to cardiology for a pericardial window procedure is determined if the patient is hemodynamically stable for the procedure. Documenting the hemodynamic instability and emergency intervention is important (see the “Documentation” box). Initial in-hospital mortality is high for patients with malignant effusion and pericardial tamponade; the median survival is 150 days, and the 1-year mortality rate is 76.5%. This mortality results jointly from the underlying cancer and the cardiovascular compromise.2
 Priority Actions
Priority Actions
• Consider malignant pericardial effusion in patients with a history of cancer who have tachypnea and dyspnea on exertion.
• Determine whether the patient has cardiac tamponade physiology by physical examination (i.e., Beck triad, pulsus paradoxus) or diagnostic evaluation (i.e., emergency bedside ultrasound).
• Perform an emergency pericardiocentesis or refer to cardiology for a pericardial window, based on hemodynamic instability.
• Assess for postprocedure reversal of tamponade physiology and for complications.
• Admit to a cardiac care or intensive care unit so that vital sign monitoring and follow-up diagnostics can be performed.
 Documentation
Documentation
• Vital signs, examination findings, and diagnostics supporting hemodynamic instability and cardiac tamponade physiology
• Informed consent for the emergency pericardiocentesis
• Postintervention assessment of vital signs, examination findings, or diagnostics to support therapeutic reversal of tamponade and improved patient clinical condition
• Code status to support the patient’s wishes given the underlying cancer history and invasiveness of the procedure
Superior Vena Cava Syndrome
Epidemiology
Currently, malignant disease is the cause of SVC syndrome in 85% of cases. Bronchogenic carcinomas account for most cases, and small cell and squamous cell carcinomas are far the most common causes. Although lung cancer is the leading cause of SVC syndrome, the overall incidence of SVC syndrome in patients with lung cancer is low, at 2% to 4%. The next most common malignant cause of the SVC syndrome is non-Hodgkin lymphoma because of its frequent presentation as a mediastinal mass. Metastatic cancers account for a small proportion of cases of SVC syndrome. Patients with SVC syndrome rarely experience immediately life-threatening complications in the absence of concurrent central airway obstruction.6,7




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


