61 Cardiac Valvular Disorders
 Key Points
Key Points• In patients evaluated in the emergency department for chest pain, dyspnea, syncope, arrhythmia, or shock, the possibility of valvular heart disease should be considered.
• Emergency echocardiography is essential in elucidating whether acute valvular pathology is responsible for hemodynamic collapse in a patient with cardiogenic shock.
• An asymptomatic patient with a grade 2/6 systolic murmur needs no further work-up.
• Diastolic murmurs are always pathologic and require echocardiography.
• Endocarditis prophylaxis is recommended only for dental procedures and no longer needed for gastrointestinal or genitourinary procedures.
Epidemiology
The American Heart Association/American College of Cardiology has published guidelines for assessment, diagnostic testing, and medical and surgical treatment of VHD.1 However, there are still many practice guidelines that are based on observational studies instead of randomized controlled trials. Recent trends in care include identifying subgroups of asymptomatic patients who may benefit from surgical intervention, valvular repair rather than replacement, and minimally invasive or percutaneous options.
Pathophysiology and Presenting Signs and Symptoms
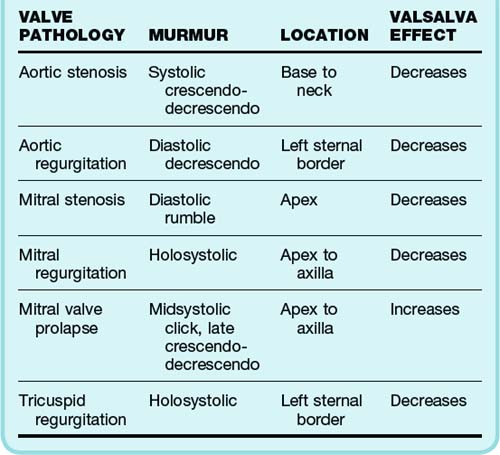
Physical examination establishes where the murmur occurs within the cardiac cycle and its location, duration, and intensity. Murmurs are classified as systolic, diastolic, and continuous. Systolic murmurs are further subclassified into holosystolic (pansystolic), midsystolic, early systolic, and late systolic. Clicks can be heard from the snapping shut of diseased valves. Diastolic and continuous murmurs are nearly always pathologic and require investigation, even in the absence of symptoms. Although many systolic murmurs merit investigation, especially those associated with symptoms, the majority of systolic murmurs do not signify valvular disease.2 A summary of the typical findings in the major valvular abnormalities is presented in Table 61.1.
Patients with midsystolic murmurs, grade 2 or less, and no associated findings or symptoms do not need any further work-up other than a history and physical examination. Aortic sclerosis is the most common defect found in these patients and requires no other intervention. However, patients with holosystolic murmurs, grade 3 murmurs, and diastolic or continuous murmurs should undergo further work-up with echocardiography.3 Some of these patients may eventually need cardiac catheterization if valve repair is planned. In patients with cardiopulmonary symptoms, detection of any new murmur warrants further investigation. The lack of a murmur in a patient with prosthetic heart valves may be pathologic and also requires further evaluation.
Differential Diagnosis and Medical Decision Making
 Priority Actions
Priority Actions
A new diastolic murmur in a patient with chest or back pain should raise suspicion for aortic dissection and requires urgent testing and consultation, as well as control of the heart rate and blood pressure.
Patients with valvular heart disease may become hemodynamically unstable with rapid atrial fibrillation and require cardioversion.
Infectious endocarditis should be considered in all patients with a prosthetic valve and fever. Blood cultures and empiric antibiotics are indicated.
Beside echocardiography should be performed in patients with shortness of breath who have recently undergone prosthetic valve replacement to rule out pericardial tamponade.
 Red Flags
Red Flags
A careful murmur examination should be performed in patients with chest pain. Individuals with severe aortic stenosis are dependent on preload to maintain systolic blood pressure, and treatment with nitrates can cause severe hypotension.
Patients in cardiogenic shock from acute mitral regurgitation, aortic regurgitation, or prosthetic valve dysfunction may not have an appreciable murmur and require emergency echocardiography. These conditions are treated surgically and will require cardiac surgery consultation.
Emergency physicians need to recognize that the absence of a murmur or mechanical heart sound is pathologic in a patient with mechanical heart valve prosthesis.
Be vigilant in patients with a bicuspid valve and chest pain because of an increased risk for aortic dissection in these individuals.
Specific Valve Lesions
Aortic Stenosis
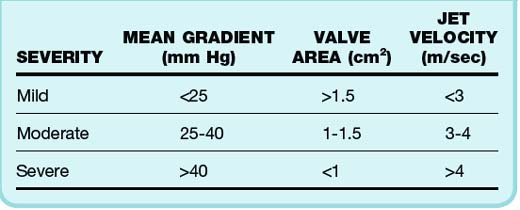
The degree of aortic valve disease is based on several factors4 (Table 61.2). Such assessment may be inaccurate and underestimate valve area and jet velocity in patients with impaired cardiac output. Progression of AS is usually quite slow, with symptoms taking decades to become manifested in most cases. An average 0.1-cm2 decrease in valve area occurs per year.5 The left ventricle is faced with systolic pressure overload and compensates through hypertrophy of the left ventricular (LV) wall. Normal chamber volume is maintained, but with increased wall thickness. The hypertrophic wall may lead to decreased coronary blood flow, even in the absence of stenosis and angina. Diastolic dysfunction and heart failure symptoms may also be present. These patients are dependent on forceful atrial contraction to maintain elevated LV end-diastolic pressure (LVEDP) to overcome the obstruction to outflow. Therefore, individuals who have AF and AS may suffer hemodynamic consequences from loss of the atrial kick.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


