CHAPTER 40 CARDIAC INJURIES
PENETRATING CARDIAC INJURY
Historical Perspective
The earliest descriptions of a cardiac injury are found in the Iliad1 and in the Edwin Smith Papyrus,2,3 written in approximately 3000 BC. Hippocrates4 stated that all wounds of the heart were deadly. Ambrose Pare,5,6 the famous French trauma surgeon, described two cases of penetrating cardiac injuries, both detailed from autopsy studies. Wolf,7 in 1642, was the first to describe a healed wound of the heart, while Senac,8 in 1749, concluded that although all wounds of the heart were serious, some wounds might heal and not be fatal. Larrey9,10 was the first to describe the surgical approach to the pericardium to relieve a pericardial effusion, and is credited with pioneering the technique for pericardial window. Billroth, in 1875 and in 1883, proclaimed his strong resistance to any attempt at cardiac injury repair.11–13 Block,14 in 1882, created cardiac wounds in a rabbit model and was successful in achieving repair, thus demonstrating successful recovery and suggesting that the same techniques could be applicable to humans. Also, Del Vecchio15 demonstrated cardiac injury healing after suturing the heart in a canine model.
However, it took the courage of Cappelen16 from Norway to attempt cardiac injury repair in a human; in 1895 he repaired a 2-cm left ventricular laceration including ligation of a large branch of the distal left anterior descending coronary artery. This was followed by Farina17 in Italy in 1896, who also attempted to repair a left ventricular wound; however, both patients succumbed. Rehn18 in Germany in 1896 was successful in repairing a wound of the right ventricle, while in the United States, Hill,19 in 1902, was the first surgeon to successfully repair a left ventricular injury.
Duval20 described the median sternotomy incision, and Spangaro,21 in 1906, described the left anterolateral thoracotomy incision. Peck22 in 1909 was the first to describe successful repair of a stab wound of the right atrium, and he reported a total of 11 patients. Smith23 was the first to develop a comprehensive plan for cardiac injury management, and for the first time pointed out the dangers of dysrhythmias occurring during cardiac manipulation. He also described the use of an Allis clamp near the apex to stabilize and hold the heart during suture placement.
Beck24 in 1942 described the technique of placing mattress sutures under the bed of the coronary arteries. During the same year, Griswold25 refined the techniques in the management of cardiac injuries and recommended that every large general hospital should have available a sterile set of instruments plus an available operating room 24 hours a day. Elkin26–28 in 1944 recommended the administration of intravenous infusions before operation and pointed to the beneficial effects of increasing blood volume and thus cardiac output. Beall and colleagues29–32 were the first to describe the technique of emergency department (ED) thoracotomy. Meanwhile, Mattox et al.33–35 refined and protocolized ED thoracotomy and cardiorrhaphy, inclusive of the use of emergency cardiopulmonary bypass in the management of these injuries. These hallmark contributions have made it possible for patients sustaining penetrating cardiac injuries to survive today.
Incidence
Feliciano et al.36 in 1983 described a 1-year experience consisting of 48 cardiac injuries at Ben Taub Hospital in Houston. Mattox and associates37 in 1989 described a 30-year experience from the same institution reporting 539 cardiac injuries (18 cardiac injuries per year). Asensio and colleagues38,39 reported two prospective consecutive series reporting a total of 165 cardiac injuries in a 3-year period (55 cardiac injuries per year) at Los Angeles County/USC Medical Center in Los Angeles. A recent review by Asensio et al.,40 which focused on the National Trauma Databank (NTDB) of the American College of Surgeons (ACS), identified a total of 2016 patients sustaining penetrating cardiac injuries, and calculated the national incidence of 0.16% for these injuries. Thus, penetrating cardiac injuries are uncommon and are usually seen only in busy urban trauma centers.
Etiology
In the civilian arena, penetrating cardiac injuries are usually caused by gunshot wounds (GSWs), stab wounds (SWs), and rarely by shotgun wounds and ice picks.41 According to a recent review,40 63% of all reported cardiac injuries in America are caused by gunshot wounds and 36% are caused by stab wounds, while shotgun and impalement injuries accounted for approximately 1% of these injuries. In the military arena, Rich and Spencer42 reported 96 cardiac injuries from the Vietnam conflict. Most of these patients sustained injuries from grenade fragments or shrapnel, while a few of these patients were impaled by flechettes.
Clinical Presentation
Beck’s triad—muffled heart tones, jugular venous distention, and hypotension—describes the classical presentation of a patient with pericardial tamponade.3,41 Kussmaul’s sign, described as jugular venous distention upon inspiration, is another classic sign attributed to pericardial tamponade. In reality, the presence of Beck’s triad and Kussmaul’s signs represent the exception rather than the rule.3,41,43 It is estimated that Beck’s triad is only present in approximately 10% of patients.41
The clinical presentation of penetrating cardiac injuries may range from complete hemodynamic instability to cardiopulmonary arrest; in fact, some penetrating cardiac injuries can be very deceptive in their presentation.41,44 The clinical presentation of penetrating cardiac injuries may also be related to factors including the wounding mechanism; the length of time elapsed before arrival at a trauma center; and the extent of the injury, which if sufficiently large in terms of myocardial destruction will invariably lead to exsanguinating hemorrhage into the left hemithoracic cavity. The presentation of these injuries is also related to blood loss, as patients who lose between 40% and 50% of intravascular blood volume develop cardiopulmonary arrest. The muscular nature of the left ventricle, and to a lesser extent that of the right ventricle, may seal penetrating injuries and prevent exsanguinating hemorrhage, allowing these patients to arrive with some signs of life at a trauma center.41,44
The most unique presentation of a penetrating cardiac injury is pericardial tamponade. The tough fibrous nature, lack of elasticity, and noncompliance of this structure translate to acute rises in intrapericardial pressure leading to compression of the thin wall of the right ventricle, impairing its ability to accept the returning blood volume, resulting in a concomitant decrease in left ventricular filling and ejection fraction. This results in a drastic decrease in cardiac output (CO) and stroke volume (SV). The impaired ability to generate both right and left ventricular ejection fractions increases cardiac work and myocardial wall tension. This results in an increase in myocardial volume of oxygen consumption (MVO2) which cannot be met, leading to myocardial hypoxemia and lactic acidosis.41,44
It is well known that the pericardium is able to accommodate gradual quantities of blood, provided that the rate of hemorrhage is slow and does not cause acute rises in intrapericardial pressures exceeding the right ventricle and subsequently the left ventricle’s ability to fill. Pericardial tamponade can have both deleterious and protective effects. Its deleterious effects can lead to a rapid rise in pericardial pressure and cardiopulmonary arrest, whereas its protective effect will limit extrapericardial hemorrhage into the left hemithoracic cavity, preventing exsanguinating hemorrhage. Moreno et al.,45 in a retrospective study consisting of 100 patients presenting with penetrating cardiac injuries, reported 77 patients who presented with pericardial tamponade. The authors reported that for patients presenting with pericardial tamponade, the survival rate was much higher—73% versus 11%—thereby ascribing tamponade a protective effect. These findings were statistically significant, leading the authors to conclude that pericardial tamponade is a critical independent factor in patient survival.
Asensio et al.,39 in a prospective 2-year study reporting 105 patients failed to find any statistical significance to the presence of pericardial tamponade in terms of survival, and were not able to identify it as a critical independent factor for survival. What remains undefined is the actual period of time after which the protective effect of pericardial tamponade is lost, and when exactly this transition occurs causing its adverse effect on cardiac function.
Diagnosis
Physical Examination
The clinical presentation of patients with penetrating cardiac injury may range from presenting hemodynamically stable to cardiopulmonary arrest. Frequently, these patients present with associated pneumohemothoraces and decreased breath sounds in the ipsilateral hemithoracic cavity. Occasionally, patients presenting with precordial injuries are restless and refuse to lie down; this may be a subtle indicator denoting the presence of hemopericardium and/or incipient pericardial tamponade. The most dramatic presentation for a patient sustaining a penetrating cardiac injury is, of course, cardiopulmonary arrest, which will require ED thoracotomy as a life-saving intervention.41,42 Pericardiocentesis is only mentioned to note that it currently has no role in establishing the diagnosis of cardiac injuries.
Subxiphoid Pericardial Window
The original technique of pericardial window was described by Larrey9,10,41 in the 1800s, and only small variations in the original technique have been added to this procedure. This technique has seen a marked diminution in its role during recent times because of the advent of two-dimensional echocardiography a part of the focused assessment and sonographic examination of the trauma patient (FAST).41 Nevertheless, the technique is still widely employed in many countries where medical personnel do not have access to ultrasound equipment.
Two-Dimensional Echocardiography
Echocardiography as part of FAST has become the gold standard in the evaluation of patients with penetrating thoracic injury. Major benefits of echocardiography include being noninvasive, rapid, and accurate; its ability to be repeated at any time; and most importantly, its painlessness. Data from two multicenter studies46,47 conclusively support the role of FAST as the initial investigative tool for the evaluation of patients with penetrating cardiac injuries, given its accuracy and ease of performance. Other techniques such as transesophageal echocardiography (TEE) have no role in the immediate evaluation sustaining penetrating precordial injuries.41
Minimally Invasive Methods
Thoracoscopy
Morales et al.48 reported a 31% incidence of positive windows describing a technique that was both accurate and well tolerated without any complications, and the authors recommend this technique to be used in patients also requiring evacuation of a retained hemothorax. In our opinion, thoracoscopic pericardial window has no role in the acute evaluation of penetrating cardiac injuries.
Management
Prehospital
Emergency medical systems in large urban areas providing rapid transport to trauma centers have allowed patients with penetrating cardiac injuries an opportunity to undergo life-saving surgical procedures. Field stabilization of patients with penetrating cardiac injuries should consist of intubation and closed cardiopulmonary resuscitation for patients found in cardiopulmonary arrest. Several studies49–52 strongly support and advocate for the need of immediate transport of patients with penetrating thoracic injuries to a trauma center, with the only predictors of outcome being the achievement of an airway via endotracheal intubation. Endotracheal intubation has been proven to increase both duration and tolerance of cardiopulmonary resuscitation administered for a period of less than 5 minutes. The return of organized cardiac electrical activity will provide the best opportunity at survival for these patients.
Emergency Department
All patients with penetrating cardiac injuries should undergo rapid initial assessment and resuscitation following Advanced Trauma Life Support (ATLS) protocols.53 Patients will usually self-stratify into those who are hemodynamically stable and may undergo diagnostic studies, those who are hemodynamically unstable but will respond to fluid resuscitation and allow for rapid transport to the operating room (OR), and those who present in cardiopulmonary arrest and will necessitate life-saving surgical interventions such as ED thoracotomy. Patients can be initially and rapidly evaluated with FAST, chest x-ray, and optionally an electrocardiogram (EKG). Volume resuscitation with lactated Ringer and O- or type-specific blood should be initiated. An arterial blood gas to determine initial pH and base deficit and lactic acid level should also be obtained. However, a significant majority of these patients will arrive “in extremis” requiring life-saving interventions.38,39,41,44
Emergency department thoracotomy
Emergency department thoracotomy is a surgical procedure of great value if undertaken after strict indications for its performance. This procedure is routinely performed in urban trauma centers that receive patients “in extremis.” When performed in an expedient fashion, ED thoracotomy, aortic cross-clamping, and cardiorrhaphy are successful in salvaging approximately 10% of all penetrating cardiac injuries. Open cardiopulmonary massage after definitive repair of penetrating cardiac injuries is more effective in producing a greater ejection fraction. Similarly, lacerations of major thoracic blood vessels can also be controlled by means of vascular clamps.41,44
Prehospital factors predictive of poor outcome include absence of vital signs, fixed and dilated pupils, absence of cardiac rhythm, absence of motion in the extremities, absence of a palpable pulse, and the presence of cardiopulmonary arrest are predictors of poor outcome.41,44
Generally accepted indications for this procedure include cardiopulmonary arrest secondary to penetrating thoracic injuries and profound shock with systolic blood pressures of less than 60 mm Hg because of exsanguinating hemorrhage or pericardial tamponade. Cardiopulmonary arrest secondary to blunt injury is generally a contraindication to the performance of this procedure.41,42,44
Objectives to be achieved with this procedure include resuscitation of agonal patients arriving with penetrating cardiothoracic injuries, evacuation of pericardial tamponade, control of massive intrathoracic hemorrhage secondary to cardiovascular injuries, prevention of air emboli, and restoration of cardiac function using open cardiopulmonary massage. Other objectives accomplished include definitive repairs of penetrating cardiac injuries and control of exsanguinating thoracic vascular injuries. Similarly, cross-clamping of the descending thoracic aorta, redistributing the remaining blood volume to perfuse the carotid and coronary arteries, is achieved with this technique.41,42,44
Emergency department thoracotomy should be performed simultaneously with the initial assessment evaluation and resuscitation, using the ATLS53 protocols by trained trauma surgeons. Similarly, immediate venous access with simultaneous use of rapid infusion techniques complements the resuscitative process. A left anterolateral thoracotomy commencing at the lateral border of the left sternocostal junction and inferior to the nipple is carried out and extended laterally to the latissimus dorsi. In females, the breast is retracted cephalad. This incision is rapidly carried through skin until the intercostal muscles have been reached and sharply transected. A Finochietto retractor is then placed to separate the ribs. The lung is then elevated medially, and the thoracic aorta is located immediately as it enters the abdomen via the aortic hiatus. The aorta should then be palpated to assess the status of the remaining blood volume. It can also be temporarily occluded digitally against the bodies of the lower thoracic vertebrae. To fully cross-clamp the aorta, a combination of sharp and blunt dissection commencing at both the superior and inferior borders of the aorta is performed, so that the aorta may be encircled between the thumb and index fingers; this facilitates the aortic cross-clamp to be placed safely. Trauma surgeons should then observe the pericardium and search for the presence of an injury. The pericardium is usually tense and discolored in the presence of tamponade. A longitudinal opening in the pericardial sac is then made anterior to the phrenic nerve and extended both inferiorly and superiorly. Usually it is necessary to grasp the pericardium and then make a small incision sharply, followed by opening the pericardium with Metzenbaum scissors.
Digital control of penetrating ventricular injuries as they are simultaneously sutured prevents further hemorrhage. We generally recommend the use of monofilament suture, such as 2-0 polypropylene. If the injury or injuries are quite large, balloon tamponade using a Foley catheter can temporarily arrest the hemorrhage either to allow the performance of cardiorrhaphy or to gain time so that the patient may be transferred expeditiously to an OR for a more definitive surgical procedure. We do not recommend the use of bioprosthetic materials such as Teflon patches in the ED. This is a time-consuming technique that, if needed, should be performed in the OR.41,44
In our experience, staples do not effectively control hemorrhage, tend to enlarge the cardiac injury, and prove to be rather difficult to remove, although they have worked in the hands of others.54
Outcomes of emergency department thoracotomy for penetrating cardiac injuries
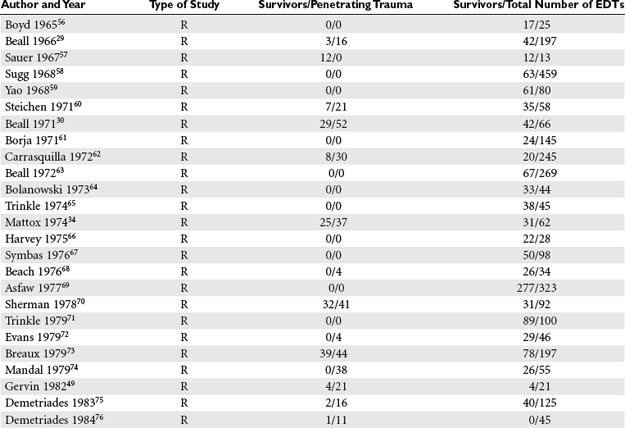
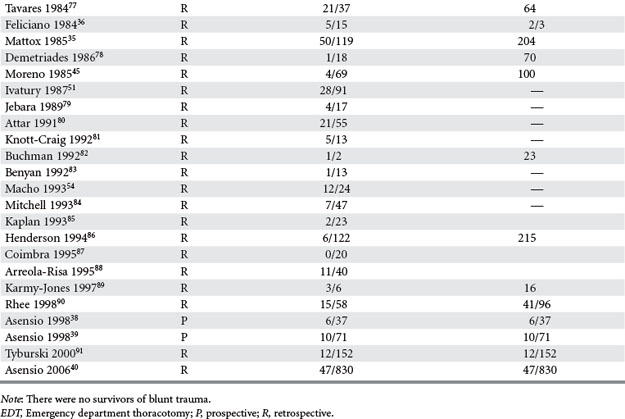
Wide disparity in the reporting of outcomes exists in the literature, ranging from 0% to 72%. Most of these series are retrospective, and the patients reported have been injured because of stab wounds. Asensio, Wall, and others in the Working Group of the Committee on Trauma of the American College of Surgeons,55 after an extensive analysis of the literature, generated practice management guidelines for ED thoracotomy (Table 1).
Techniques for Cardiac Injury Repair
Incisions
Two main incisions are used in the management of penetrating cardiac injuries. Median sternotomy described by Duval20 is the incision of choice for patients admitted with penetrating precordial injuries that arrive with some degree of hemodynamic instability and may either undergo preoperative investigation with FAST and/or chest x-ray. The left anterolateral thoracotomy described by Spangaro21 is the incision of choice in the management of patients who arrive “in extremis.” This incision is used in the ED for resuscitative purposes, and it can also be extended across the sternum as bilateral anterolateral thoracotomies. Extension into bilateral anterolateral thoracotomies is also the incision of choice for patients who are hemodynamically unstable after incurring mediastinal-traversing injuries (Figure 1). It is important to note that upon transection of the sternum, both internal mammary arteries are also transected and must be ligated after restoration of perfusion pressure. For patients who sustain thoracoabdominal injuries, the left anterolateral thoracotomy is also the incision of choice if patients deteriorate in the OR while undergoing a laparotomy.44,92
< div class='tao-gold-member'>
Related posts:
 THE DEVELOPMENT OF TRAUMA SYSTEMS
THE DEVELOPMENT OF TRAUMA SYSTEMS
 DELIVERING MULTIDISCIPLINARY TRAUMA CARE: CURRENT CHALLENGES AND FUTURE DIRECTIONS
DELIVERING MULTIDISCIPLINARY TRAUMA CARE: CURRENT CHALLENGES AND FUTURE DIRECTIONS
 GASTRIC INJURIES
GASTRIC INJURIES
 PALLIATIVE CARE IN THE TRAUMA INTENSIVE CARE UNIT
PALLIATIVE CARE IN THE TRAUMA INTENSIVE CARE UNIT
 TRAUMATIC BRAIN INJURY: PATHOPHYSIOLOGY, CLINICAL DIAGNOSIS, AND PREHOSPITAL AND EMERGENCY CENTER CARE
TRAUMATIC BRAIN INJURY: PATHOPHYSIOLOGY, CLINICAL DIAGNOSIS, AND PREHOSPITAL AND EMERGENCY CENTER CARE
 NOSOCOMIAL PNEUMONIA
NOSOCOMIAL PNEUMONIA
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


