The heart is a pump with an electrical controlling system. Its power supply comes from burning fuel with oxygen. It stops functioning in three main ways:
Asystole is the final rhythm in all cases. The underlying causes of the three arrest rhythms are described below.
Asystole
Similar to any other pump, the heart slows and stops when deprived of its power supply. This results from:
- hypoxia or
- a condition leading to hypoxia (e.g. hypovolaemia).
Tachycardia during hypoxia is the result of the influence of the autonomic nervous system. Left to its own devices, the hypoxic heart contracts more slowly (terminal bradycardia) and then arrests in asystole.
Ventricular Fibrillation
Ventricular fibrillation is caused by direct damage or irritation of the heart. This may be because of:
- myocardial ischaemia or infarction
- poisoning
- gross electrolyte imbalance
- hypothermia and near drowning
- electrocution
- penetrating trauma
- iatrogenic causes (e.g. cardioversion and cardiac catheterisation).
In adults VF is most commonly seen in patients with ischaemic heart disease whereas, in children, poisoning with tricyclic antidepressants should always be considered. Pulseless VT is a similar condition to VF in both causation and treatment. Unfortunately, these ‘shockable’ rhythms occur less than half the time, accounting for only 40% of prehospital cardiac arrests and 25% of arrests in hospital.
Pulseless Electrical Activity
Pulseless electrical activity is that state when the pump (the myocardium) is unable to function despite a relatively normal electrical stimulus (the ECG signal). This can be because of primary damage to the cardiac muscle including:
- extensive myocardial infarction
- ruptured cardiac aneurysm
- papillary muscle rupture
- extreme direct trauma
or because of various secondary causes (some of which may be treatable):
- tension pneumothorax
- cardiac tamponade
- pulmonary embolism (PE)
- hypovolaemia
- hypothermia
- poisoning
- electrolyte imbalance.
In adults, myocardial infarction (MI) is the most common cause of PEA, whereas hypovolaemia should be suspected in children. PEA should not be confused with an agonal rhythm (→ p. 161).
The Chain of Survival
Survival from cardiac arrest is most likely if:
- the arrest is witnessed (and recognised!)
- the initial rhythm is VF (or VT).
Thereafter, the chain of survival depends on the patient receiving the following:
Complete failure of the circulation for more than 3 or 4 minutes leads to irreversible brain damage.
There are only three interventions that are known to increase the survival from cardiac arrest: chest compression, defibrillation and airway management. The aim of life support must be to deliver these three treatments to the patient in the shortest possible time.
Cardiac Arrest in Children
Children’s hearts usually arrest as a result of hypoxia secondary to respiratory distress or depression, or hypovolaemia (fluid loss or maldistribution). These conditions lead to asystole, which has a very poor prognosis. Coronary artery disease and thus VF are extremely uncommon in children.
Basic Life Support
Figure 11.1 Basic life support for adults.
Reproduced with the kind permission of the Resuscitation Council (UK).
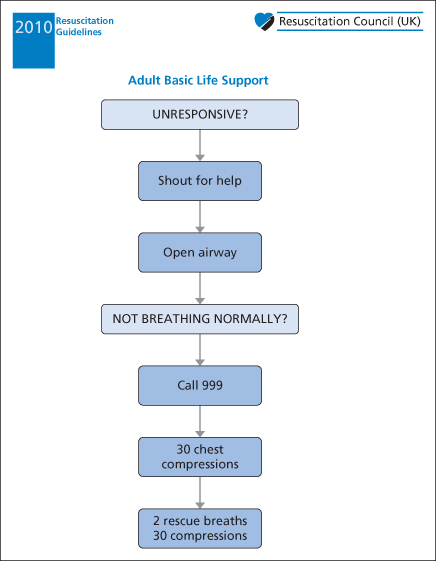
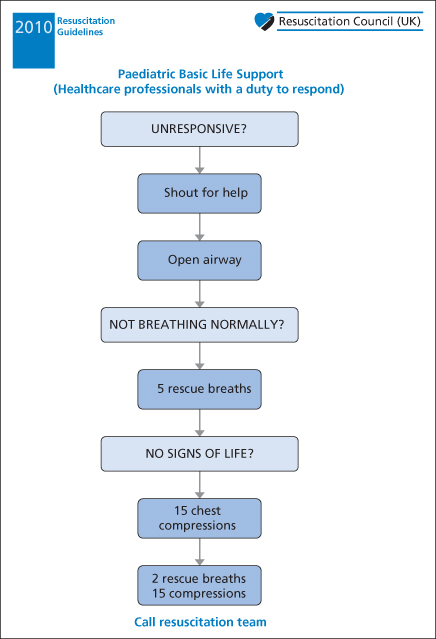
Figure 11.2 Basic life support for children.
Reproduced with the kind permission of the Resuscitation Council (UK).
The manual methods of BLS (Schafer’s, Silvester’s and the Holger–Nielsen procedures) were replaced by exhaled air resuscitation in the late 1950s. In 1960, Kouwenhoven, Jude and Knickerbocker reminded the world of the efficacy of closed chest compression and thus modern BLS was born. There are four elements:
Basic life support is not very effective – even optimal chest compressions do not achieve more than 30% of the normal blood flow to the brain and 15% of the normal coronary blood flow. It is thus essential to restart the heart within a few minutes (→ The chain of survival above).
In adults, arrest is usually a primary cardiac event and so most effort relates to obtaining a defibrillator as soon as possible, even if this means leaving a pulseless patient to go to a telephone before starting chest compressions. Minimally interrupted chest compressions are then the primary focus of BLS. In children, more attention is given to the correction of hypoxia and so resuscitation, starting with five rescue breaths, should be performed for about 1 minute before an isolated rescuer goes for help. (The exception to this recommendation is a child with a sudden witnessed collapse when a shockable rhythm is more likely.) Adults who are victims of drowning should also be given five breaths and a short period of cardiopulmonary resuscitation (CPR) before seeking assistance. BLS for adults is now taught assuming one rescuer who will perform sequences of 30 compressions to 2 ventilations. Two-rescuer CPR (using the same compression : ventilation ratio of 30 : 2) is taught to professionals only. For children, the 30 : 2 ratio is taught to lay rescuers but two or more health professionals should use a 15 : 2 sequence. The only exception is neonates where a 3 : 1 ratio of compressions to ventilations is advocated. After successful endotracheal intubation, the synchronisation of compression and ventilation is abandoned and the two operations are performed independently.
Initial Assessment
- Make sure that the victim, any bystanders and yourself are safe.
- Shake and shout ‘Are you alright?’.
- If the patient is responsive, leave them in the position found (or in the recovery position if safer), try to find out what is wrong and get help. Review the situation regularly.
- If the patient is unresponsive, call for help (or go for help if alone). Turn the victim on to his or her back, open the airway and, in less than 10 seconds, look for chest movements, listen at the mouth for sounds and feel for air flow on your cheek.
- If the patient is breathing normally, turn him or her into the recovery position, get help and continue monitoring the situation.
- If the patient is not breathing, call for help (or go for help if alone) and then start chest compressions.
Chest Compression
Even the best external chest compression provides poor core circulation. Squeezing the chest results in cardiac valve deformation and incompetence which allows regurgitation of blood into the inferior vena cava. Retrograde flow up the superior vena cava is reduced by a valvular effect where the superior vena cava enters the chest. Forward flow to the brain is thus more likely to occur than forward flow to the trunk. In contrast, coronary artery perfusion, which normally occurs only in diastole against a closed aortic valve, is very poor during BLS. A coronary perfusion pressure <15 mmHg has been shown to be unlikely to lead to a return of spontaneous circulation and the average coronary perfusion pressure during manual CPR is only around 12.5 mmHg.
The mechanism by which BLS produces cardiac output remains unclear; there is probably a combination of direct cardiac compression and intrathoracic pressure fluctuations. Their relative importance may vary between individuals, depending on the shape and elasticity of the chest. At the current time, Resuscitation Council teaching assumes that direct cardiac compression is the most important factor – hence the emphasis on correct site and adequate depth. A compression rate of about 100/min is recommended for both adults and children. The weight of the resuscitator’s body is transmitted through the arms to achieve a compression of 4–5 cm in normal adults or about a third of the depth of the chest in children. The compression : release ratio should be 1 : 1. The current guidelines aim to reduce the interruptions in chest compression that occur for ‘rescue breaths’ by advocating a compression : ventilation ratio of 30 : 2. Pauses for ventilation should be limited to 1 s/breath only. For children, the same ratio of 30 : 2 is appropriate for lay rescuers but a 15 : 2 sequence should be used when two or more health professionals are present. The only exception is neonates where a 3 : 1 ratio of compressions to ventilations is advocated. After successful endotracheal intubation, the synchronisation of compression and ventilation is abandoned and the two operations are performed independently.
Ventilation
Five initial ‘rescue breaths’ are recommended for children whereas, for adults, the 2 first breaths are given only after the first 30 chest compressions. Each breath should only take 1 second so as to maintain constant chest compressions. Mouth to mouth-and-nose ventilation is required for infants. A pocket mask may be used by occasional resuscitators to avoid direct patient contact; professional rescuers should use bag, valve and mask units initially but aim for endotracheal intubation as soon as practically possible. Airway adjuncts such as the oesophageal obturator airway and Combitube are not recommended – there are more disadvantages to their use than advantages. However, the laryngeal mask airway (LMA) is increasingly used by first responders.
Advanced Life Support
These protocols apply, by definition, to healthcare professionals trained in advanced life support techniques.
Figure 11.3 Advanced life support for adults.
Reproduced with the kind permission of the Resuscitation Council (UK).
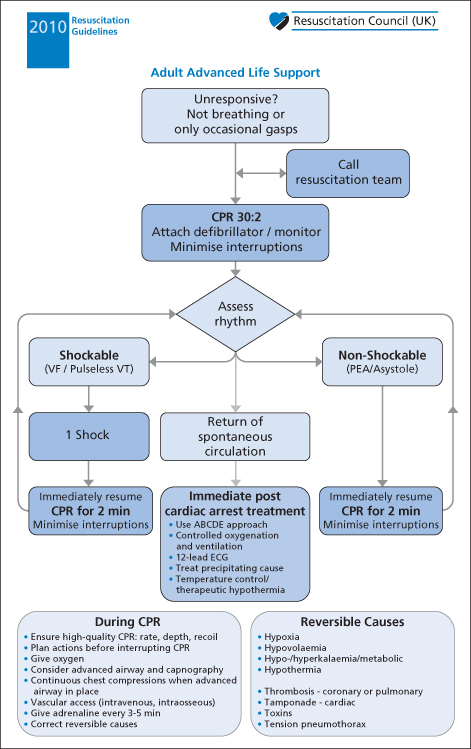
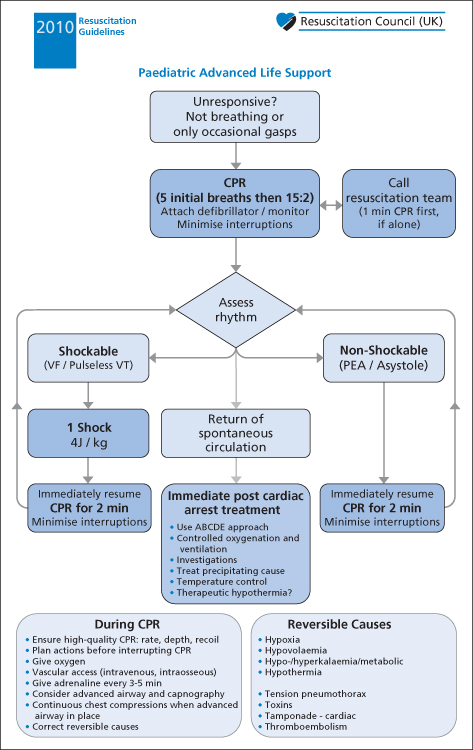
Figure 11.4 Advanced life support for children.
Reproduced with the kind permission of the Resuscitation Council (UK).
A display of the ECG must be obtained as soon as possible to guide treatment. Monitoring via defibrillator pads (or paddles) may be adequate initially but should be replaced by adhesive chest electrodes once ALS is established. Endotracheal intubation must be achieved as soon as practically possible and early venous (or intraosseus) access is also desirable. Once the airway has been secured with a cuffed endotracheal tube, compressions should not be interrupted for ventilations. From then on, ventilation of the lungs should be performed asynchronously at a rate of approximately 10–12 breaths/min. To ensure effective chest compressions, the person responsible for this tiring part of the resuscitation should be changed every 2 min at least.
With the aid of the ECG rhythm, the algorithms divide patients into two categories: those who have VF or pulseless VT and those who do not have VF or VT. VF is not the most common arrest rhythm but is the most survivable by far. The only effective treatment for it – defibrillation – was introduced into clinical practice by Zoll and colleagues in 1956. In almost all circumstances, no other intervention must take precedence over defibrillation.
Precordial Thump
This supplies energy that may abort VT or even VF but in the unstable heart it may also possibly convert sinus rhythm into VF. Therefore, its use is recommended only in witnessed arrests when ALS skills are available.
Gastric Decompression
Inflation of the stomach is inevitable during BLS. It causes splinting of the diaphragm and may impair cardiac output. For this reason, it is helpful to decompress the stomach with a large-bore orogastric (lavage-type) tube as soon as possible during all resuscitations. This should not be attempted until the airway is protected by intubation. The stomach may be emptied of both air and fluids in order to decrease the risk of aspiration. At postmortem examination, almost half of all patients who have died after attempted resuscitation are found to have full stomachs. Contamination of the respiratory tract is evident in 30%. Airway protection is ensured by early endotracheal intubation; the LMA is an effective alternative for first responders.
Relatives
Honest, accurate and frequent communication with relatives is essential throughout all resuscitations. Increasingly, relatives are being encouraged to come into the resuscitation room, even if it is only for a very short period. Staff may feel threatened by their presence but relatives are reassured by the experience; however cluttered and confusing the resuscitation area may appear, the reality is often less frightening than their imaginings. A dedicated member of staff should accompany relatives in the resuscitation room at all times.
Drugs in Advanced Life Support
Adrenaline
The vasoconstrictor adrenaline is known to enhance both myocardial and cerebral perfusion, although there is no evidence that it increases the survival to hospital discharge in cardiac arrest. It has a very short half-life and so repeated intravenous (IV) doses (1 mg for adults) are given every 3–5 min during CPR. In children, the corresponding IV/intraosseous (IO) dose is 10 mcg/kg. Adrenaline should be given as soon as circulatory access is obtained in non-shockable rhythms and after the third shock (once chest compressions have been resumed) in shockable rhythms. Adrenaline may be contraindicated in arrests secondary to solvents, cocaine or other sympathomimetic drugs.
Amiodarone
Amiodarone is given for refractory VF/pulseless VT after the third shock (once compressions have been resumed). It stabilises cell membranes and thus increases the duration of the action potential and refractory period in both atrial and ventricular myocardial cells. As an antiarrhythmic agent, it prolongs the Q–T interval and slows conduction through both the atrioventricular (AV) node and any accessory pathways. Amiodarone has less negative inotropic effects and fewer proarrhythmic actions than most similar drugs. An initial IV bolus of 300 mg should be given in adults; the equivalent IV/IO dose for children is 5 mg/kg. A further dose of 150 mg may be given for persistent or recurrent VF/VT, followed by an infusion of 900 mg over 24 h.
Atropine
Atropine is no longer recommended in cardiac arrest. Pulseless patients with extreme bradycardia or isolated P waves may benefit from pacing (→ p. 160).
Bicarbonate
Bicarbonate therapy is contraindicated in early resuscitation. Acidosis develops but aids oxyhaemoglobin dissociation; temporary buffering of pH is achieved by hyperventilation. Sodium bicarbonate is reserved for cardiac arrests that are associated with the following:
The initial dose is 50–100 mmol (or 1–2 mmol/kg). Further information about bicarbonate therapy → Box 14.24 on p. 252. Prolonged arrest (i.e. over 20–25 min) causes profound intracellular acidosis and so may also be treated with alkalising agents, especially in children.
Lidocaine
Lidocaine reduces ventricular automaticity and ectopic activity and increases the threshold for the development of VF. However, it also causes an increase in:
- the energy required for defibrillation
- the incidence of post-shock asystole.
In addition, it is a negative inotrope. For these reasons, it is not routinely used for refractory VF/VT unless amiodarone is unavailable. The initial IV/IO dose for both adults and children is 1.0–1.5 mg/kg to a maximum total dose of 3 mg/kg in the first hour. Lidocaine and amiodarone should not be used together.
Magnesium
Magnesium is an important intracellular cation and co-factor. It should be given for refractory VT that could be associated with low serum magnesium levels, e.g. in a patient known to be taking potassium-losing diuretics. Similar indications include arrests after episodes of torsade de pointes or in patients with digoxin toxicity. The usual dose of magnesium sulphate is 8 mmol (2 g or 4 mL of a 50% solution). For children, the dose is 25–50 mg/kg by IV infusion over several minutes. These doses may be repeated after 10–15 min.
Calcium
Calcium influx occurs at the time of cell death and thus it is illogical to give calcium to patients in cardiac arrest. Exceptions occur during resuscitation from PEA or asystole when there is thought to be one of the following conditions:
The initial IV dose in these situations is 10 mL of 10% calcium chloride (6.8 mmol calcium ions), repeated as necessary. For children the dose of 10% calcium chloride solution is 0.2 mL/kg. Calcium may form a precipitate if given in the same IV line as bicarbonate and is dangerous in the digitalised patient. Calcium channel blocking drugs have not fulfilled their early promise and do not improve outcome after cardiac arrest.
Drugs in Cardiac Arrest After Hypothermia
Drug metabolism is reduced in hypothermia and toxic accumulation of drugs may thus occur. For this reason, it is usually recommended that adrenaline and other drugs are withheld until the patient’s core temperature reaches 30°C. At this point, the interval between drug doses is doubled (adrenaline is given every 6–10 min) until a core temperature of around 35°C has been reached.
Ventricular Fibrillation and Pulseless Ventricular Tachycardia
In adults, VF/VT is the most treatable cause of cardiac arrest. Cardioversion by DC shock is most likely to be successful if carried out within 90 s of cardiac arrest. Thereafter, the chances of success decline at a rate of about 7–10%/min. Nevertheless, repeated shocks are delivered until sinus rhythm is established or resuscitation is abandoned. First and all subsequent shocks are delivered with an energy level of 360 J (or 4 J/kg) from a monophasic source. However, when using a modern biphasic defibrillator, fixed or escalating energies of between 150 and 360 J (4 J/kg for children) are recommended (→ Table 11.2).
The largest possible size of paddle (electrode) should be used for all DC shocks. There are three diameters currently available (→ Table 11.3). Size is limited by the two following criteria:
Self-adhesive electrode pads are likely to replace defibrillator paddles completely in the near future.
Single shocks are given every 2 min. After administering a shock, there should be no delay in resuming CPR. It will not harm the patient if the defibrillation has been successful and the circulation has returned. The central pulse is checked only if the clinical condition of the patient changes or if the ECG shows a rhythm that is compatible with a cardiac output. (The carotid pulse is used in adults and children aged >12 months but in infants the brachial pulse is more appropriate.) After three unsuccessful shocks, adrenaline and amiodarone should be given. Further doses of adrenaline are given every 3–5 min throughout the resuscitation, immediately after alternate shocks (→ Table 11.1).
Table 11.1 Doses of adrenaline and amiodarone for adults and children in cardiac arrest
| Adrenaline (to be given as soon as possible in asystole/PEA and after the third shock in VF/VT) | Amiodarone (to be given after the third shock in VF/VT) | |
| Adult | 1 mg every 3–5 min | 300 mg |
| Child | 10 mcg/kg every 3–5 min | 5 mg/kg |
All dosages are the same whether the drugs are given by the intravenous or intraosseous route.
10 mcg/kg of adrenaline = 0.1 mL/kg of 1 in 10 000 solution.
Peripheral IV or IO doses should be flushed in with saline.
Table 11.2 Doses of electricity for adults and children in VF or pulseless VT
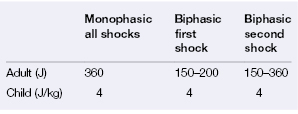
Table 11.3 Suggested paddle diameters for DC shock
| Size of patient | Diameter of paddle (cm) |
| Infants (i.e. weight <10 kg) | 4.5 |
| Children aged <8 years (i.e. weight <25 kg) | 8 |
| Adults and children aged >8 years | 13 |
Potentially reversible causes of cardiac arrest must always be considered (→ Box 11.1). Underlying non-cardiac causes of VF are more likely to be found in children than in adults. Magnesium should be considered if there is any suspicion of hypomagnesaemia (→ p. 174). If attempts at defibrillation remain unsuccessful, a change of paddle positions or a change of machine should be considered. Alternatives to the traditional anteroapical (AA) positioning of electrodes include anteroposterior (AP) and biaxillary (LL) placement. The latter positions (LL) should always be employed in patients with a pacemaker in situ.
 Box 11.1 Potentially Reversible Causes of Cardiac arrest (‘the 4 Hs and 4 Ts’)
Box 11.1 Potentially Reversible Causes of Cardiac arrest (‘the 4 Hs and 4 Ts’)After Successful Defibrillation
After successful defibrillation (if it has not already been utilised), amiodarone may be given to stabilise the myocardium and prevent a return to VF/VT. The IV dose is 300 mg over 20–60 min followed by an infusion of 900 mg over 24 h. Lidocaine (which also raises the fibrillation threshold) is a further option. The dose is 100 mg for an average adult followed by an infusion of 2–4 mg/min.
Safety of Staff
This is paramount during attempts at defibrillation and requires:
- a good knowledge of the equipment
- a warning shout of ‘stand clear’ and a visual check before each discharge.
The use of adhesive electrode pads makes the procedure much safer and better controlled.
Defibrillation in Cardiac Arrest After Hypothermia
VF may not respond to defibrillation if the patient’s core temperature is <30°C. Thus it is usually recommended that, if there is no response to the first three shocks, subsequent attempts at defibrillation are delayed until the core temperature rises above 30°C.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


