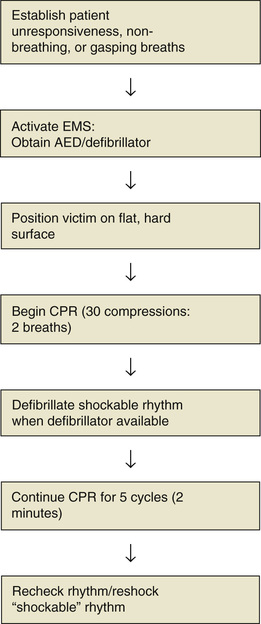
Terry Mahan Buttaro According to the American Heart Association (AHA), 17.3 million people in the world die each year from heart disease.1 In the United States, cardiovascular disease is the cause of one of three deaths annually, and it is important to realize that out-of-hospital sudden deaths affect children as well as adults and elders.1 What is startling is that most sudden deaths in young athletes are related to cardiovascular disease.1 The majority of these events (82%) in young athletes occur during physical exertion while training or participating in competitive sports.1 Unfortunately, despite the important research and information available about coronary artery disease (CAD), our efforts to combat this disease and provide education on cardiopulmonary resuscitation (CPR), sudden cardiac death remains a significant cause of cardiac-related death. Only 10.6 % of those who have an out-of-hospital cardiac arrest survive, and only 8.3% have good neurologic outcomes.1 If the event is witnessed, one of three victims of sudden cardiac arrest survives.1 Equally concerning is the awareness that the incidence of out-of-hospital arrest and survival is less for blacks and Hispanics than for whites.1 Many out-of-hospital cardiac arrest victims seem symptom free before the event occurs, and, surprisingly, only 23% have a shockable cardiac rhythm (i.e., ventricular tachycardia, ventricular fibrillation) when the cardiac arrest occurs.2 The importance of immediate cardiac resuscitation is evident, particularly because survival rates for out-of-hospital arrests continue to be low.2 Whether cardiac arrest occurs in the hospital, in the office, or in the community, resuscitative efforts should be initiated immediately.3 Trained health care professionals should immediately initiate resuscitation to maintain circulation, airway, and breathing (CAB) until advanced life support (ALS) is available (Fig. 28-1).3 Preplanning is essential. Health care providers should be trained in basic CPR as well as in acute life support. In addition, each member of the office team should have a specified role if a cardiac arrest occurs in the office or clinic setting. If available, intramuscular or intranasal naloxone is appropriate if an unresponsive victim is not breathing, has a pulse, and is suspected to be opiate addicted. Cardiac arrest may result from either cardiac causes or extraneous circumstances. The net effect is the cessation of cardiac rhythm and the resultant tissue hypoxia and acidosis. Biologic death will occur if resuscitative measures are not instituted immediately. There may be no warning that an acute event is about to occur. Presentation can include the classic midsternal, crushing, viselike chest pressure with radiation to the arm, neck, or jaw and accompanying diaphoresis, or it may consist of vague, nonspecific symptoms that include chest tightness, discomfort, nausea, shortness of breath, palpitations, lightheadedness, or syncope. A recent history of angina, fatigue, and other nonspecific complaints is also frequently reported. A medical history of smoking, hypertension, elevated cholesterol level, diabetes, sedentary lifestyle, and family history of CAD are significant risk factors for cardiac arrest; therefore it is beneficial to obtain this information.2 If information cannot be elicited from the patient, family members or others should be questioned to determine the patient’s medical history and details of the circumstances surrounding the event. Assessing unresponsiveness in a calm but efficient manner is critical in the initial management of cardiac arrest. Determining breathlessness and pulselessness in less than 10 seconds is crucial. Once breathlessness and/or pulselessness is confirmed, the resuscitation team or emergency medical services (EMS) system should be activated to enable rapid procurement of an automated external defibrillator (AED) or a conventional defibrillator. If a second person is available to activate the EMS system, the primary provider should place the victim in a supine position on a hard, firm surface. The AHA recommends ensuring scene safety, determining if the victim is not breathing, has “gasping” breaths, or no pulse and then calling for help and activating the Emergency Response System (using a mobile phone is rapid and efficient), simultaneously with beginning CPR.3 A search for a pulse should not exceed 10 seconds to avoid delaying chest compressions.4 If the victim has a pulse, but is not breathing, a rescue breath every 5 to 6 seconds is indicated. If there is no pulse, begin CPR. The compression rate should be 100 to 120 compressions per minute, the compression depth for an adult patient should be 2 inches, but not more than 2.4 inches, and interruptions to compressions must be minimumized (<10 seconds) throughout the resuscitation effort.3 The chest should be allowed to fully recoil between compressions. Health care professionals and trained rescuers should provide two ventilations for every 30 compressions, but rescuers who are not trained are encouraged to provide chest compressions only. For trained rescuers, ventilations can be started after chest compressions have been initiated, although the time interval without chest compressions should be minimal.3 After the initial 30 chest compressions have been performed, the approach to providing ventilations to the victim consists of opening and inspecting the airway with the head tilt–chin lift or jaw thrust (if trauma is suspected) maneuver. The rescuer will use mouth to mask or a bag mask device to provide ventilation and oxygen to the victim. The breath is given during 1 second and should have enough volume to make the chest rise. The chest should be allowed to recoil completely after the compression. Once the chest recoils, the second breath is given. If the chest does not rise, the rescuer should reposition the victim’s head and attempt another breath. The resuscitation effort is continued with at least 100 to 120 compressions per minute, and a compression depth of (2 to 2.4 inches, 30 compressions to two breaths). The AHA recommends minimal interruptions to CPR and that victims of a witnessed arrest be defibrillated as soon as possible (preferably within 3 to 5 minutes),3 but CPR is administered until the AED or defibrillator is available and ready. As soon as an AED or conventional defibrillator is available, the leads are attached to the victim, the rhythm is assessed, and, if appropriate, the victim is defibrillated according to AHA standards (see Fig. 28-1).3 For victims with an implantable pacemaker or implantable cardioverter-defibrillator (ICD), the recommendation is to not place the AED or defibrillator pads or paddles over the device.4 If a monophasic defibrillator is used, the recommended energy level is 360 J for all shocks.5 If a biphasic defibrillator is used, the recommendation is 120 to 200 joules.4 Once the defibrillator is attached, one shock should be given if the rhythm is a shockable rhythm. CPR should then immediately commence again and continue for five cycles of CPR (about 2 minutes).4 At the end of each five-cycle sequence (after the 30 compressions), the rhythm should be reassessed and the patient again defibrillated for a shockable rhythm.4 Pulse checks by health care providers should not exceed 10 seconds. If the arrest was not witnessed, a precordial thump is not recommended.6 As soon as an AED or conventional defibrillator is available, the leads are attached to the victim, the rhythm is assessed, and, if appropriate, the victim is defibrillated according to AHA standards (see Fig. 28-1).3 If the patient’s own defibrillator is activated, the rescuers should wait 30 to 60 seconds before the AED is placed on the patient and activated.4 In a witnessed arrest, the AHA considers the precordial thump to be a “consideration” for health care providers if the victim is monitored and in unstable ventricular tachycardia and if a defibrillator or AED is not available.6 Continued assessment of the resuscitation efficacy—compression rate and depth, airway maintenance, and the need for defibrillation—is ongoing. At frequent intervals, the provider should reassess heart rate, blood pressure, oxygen saturation, and effectiveness of CPR and defibrillation.
Cardiac Arrest
Definition and Epidemiology
 Immediate emergency department referral or physician consultation is indicated for cardiac arrest.
Immediate emergency department referral or physician consultation is indicated for cardiac arrest.
Pathophysiology
Clinical Presentation
Physical Examination
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


