127 Breast Disorders
 Key Points
Key Points• There are very few true breast emergencies, and immediately life-threatening causes such as traumatic breast rupture or necrotizing fasciitis are exceedingly rare.
• Breast pain, particularly if cyclic, is common, and benign causes predominate.
• Breast cancer is a possible diagnosis in any patient with a chief complaint related to the breast, including breast pain or a mass, nipple discharge, or skin lesions.
• Most patients in whom breast cancer is diagnosed have no risk factors except age older than 50 years and female sex, and eight of nine patients have no family history of breast cancer.
• The emergency physician can play a role in reduction of the risk for lymphedema by early and aggressive treatment of even very minor infections and burns.
• Most medications are safe for use while breastfeeding, and the benefits of continuing breastfeeding generally outweigh the potential for harm.
• Few maternal infections, other than human immunodeficiency virus, present a significant risk to the breastfeeding infant.
Acknowledgment and thanks to Dr. Karen Jubanyik for her contribution to the first edition.
Epidemiology
Approximately one half of visits to physicians for breast complaints are for pain. New, palpable masses represent another common breast-related complaint. Although a benign condition will be diagnosed in 9 of 10 premenopausal women with a palpable breast mass, a new mass in a 75-year-old woman is malignant up to 70% of the time. Breast cancer is the most common cause of cancer-related mortality in women worldwide and second only to lung cancer in women in the United States. In 2006, it accounted for one third of all cancer diagnoses in women in the United States.1
Although there are few true breast-related emergencies, perioperative issues represent a second significant group of emergency department (ED) visits. Breast surgery is relatively common in the United States. In addition to the 90,000 mastectomies performed annually, approximately 100,000 cosmetic augmentations and 100,000 reduction mammoplasties take place each year.2 Many patients undergoing breast augmentation, either for reconstruction or cosmesis, experience significant complications and require additional surgery.
Pathophysiology
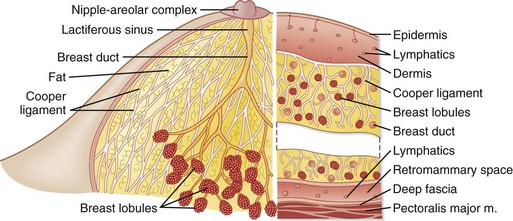
The unique anatomic structure of the breast contributes to the wide variety of pathologic conditions that may occur. Each breast contains approximately 20 glandular units (lobes) composed of glands and adipose tissue (Fig. 127.1). Each lobe drains into a lactiferous duct, which fuses with other ducts to form lactiferous sinuses just below the skin. The lactiferous sinuses store milk during lactation. Disruption (obstruction, infection, inflammation) of the glandular system may occur at any time during a female’s lifetime but predominates between menarche and menopause. The breast’s diffuse vascular network predisposes it to hematogenous spread of malignancy, as well as infection.
Differential Diagnosis and Medical Decision Making
See Box 127.1 for an overview of causes of breast-related complaints.
Mastalgia
Noncyclic mastalgia may be caused by a variety of conditions3 (Box 127.2). It may be constant or intermittent, but it is not associated with the menstrual cycle. Noncyclic mastalgia tends to be unilateral and localized to a discrete area. Women with noncyclic breast pain are generally older than 40 years, and the cause is likely to be related to an anatomic lesion in the breast. It is rare for breast cancer to have pain as the sole initial symptom.4
Mondor disease (Fig. 127.2) is a superficial phlebitis of the lateral thoracic, thoracoepigastric, or superior epigastric vein. It typically occurs in middle-aged women. The condition can be unilateral or bilateral. It is often idiopathic but may be associated with other conditions.5 The classic Mondor cord is 2 to 3 mm in diameter and typically red and tender, tracks from the lateral margin of the breast across the costal margin, and extends from 2 to 30 cm. Any tenderness should resolve within weeks, but the cord may remain palpable for up to 6 months. There is no risk for systemic embolization.

Dermatologic Changes and Discharge
A wide variety of skin conditions can affect the breast, nipple, or both; the most threatening and most common are listed in Box 127.3 and are discussed in the following sections.
Nonpuerperal Mastitis and Abscess
Periductal mastitis may be confused with cellulitis, abscesses, or inflammatory breast cancer. Approximately 90% of nonpuerperal breast abscesses are subareolar.6







