BOMB AND BLAST INJURIES
Blast injuries using conventional weapons have emerged as the terrorist weapon of choice. Terrorist attacks have increased dramatically over the last decade. The National Counterterrorism Center reported more than 14,000 terrorist attacks in 2007, with 44,000 injuries and 22,000 deaths, which was a 20% to 30% increase over 2006.1 Explosive devices in military conflicts have killed or injured more than 25,000 U.S. and Coalition forces and more than 100,000 Iraqis.1 Blast injuries are increasing in the civilian setting, particularly suicide bombings, and emergency personnel must be familiar with the management and treatment of blast injuries, ad potential mass casualty incidents.2,3,4,5,6,7,8,9 The United States is not immune from intentional bombings, with about 36,000 bombing incidents reported from 1983 to 2002 – including explosive, incendiary, premature, and attempted bombings.6 There were 281 injured in the 2013 Boston Marathon bombing, with most injuries involving the lower extremities and soft tissue.8 Death, survival, and hospitalization rates vary greatly, depending on the type of explosive, distance from the explosion, and whether the explosion occurred in an open or closed space. Although some victims die immediately at the scene, the majority of injuries suffered by the immediate survivors of bombings are potentially survivable. Blast injuries commonly occur not as isolated incidents, but as part of multiple-casualty incidents of varying sizes. This pattern, combined with the fact that most emergency physicians have never encountered a blast injury victim or a true mass casualty incident, makes the care of often eminently salvageable victims contingent upon appropriate training and skill retention by the individual emergency physician, along with appropriate institutional leadership, planning, and preparation.
Terrorist bombings result in high injury scores for victims as well as higher hospital resource use by victims than by victims of other trauma. Blast victims have increased immediate scene mortality, greater hospital mortality, more frequent need for surgical intervention, longer hospital stays, and greater use of critical care.
An explosion is the instantaneous transformation of a solid or liquid into a gas, releasing tremendous kinetic and heat energy. Detonation of a conventional high explosive generates a blast wave that spreads out from the detonation point and displaces air, water, or anything in its path. The blast wave consists of two parts: a shock wave of high pressure followed closely by a blast wind, which is air mass in motion. The blast wave loses its energy over distance and time.
There are four main types of blast effects. A primary injury is caused by a direct effect of blast wave overpressure on tissue. Primary blast injury mostly (but not exclusively) affects air-filled structures such as the lungs, ears, and GI tract, by the following mechanisms: spalling, shearing, and implosion. Spalling is displacement and fragmentation of a dense medium into a less dense medium.10 An example is a blast wave causing the lung parenchyma to explode into the alveolar space like a geyser. Shearing, sometimes called inertia, is a stress caused by the blast wave traveling through different tissue densities at different velocities. An example of shearing is the blast wave traveling through the pulmonary vessels and air spaces, resulting in ruptured vascular and bronchial pedicles. Implosion is the opposite of spalling, where the less dense material is displaced into denser material. An example of implosion is the blast wave causing the flexible air spaces to rebound to greater than original size, sometimes causing air embolism from the alveoli into the pulmonary vessels.10 A secondary blast injury is due to collateral damage from flying objects and shrapnel (Figures 7-1 and 7-2). Tertiary blast injury results from the victim being propelled through the air and striking stationary objects. A quaternary blast injury is a result of burns, smoke inhalation, or chemical agent release.
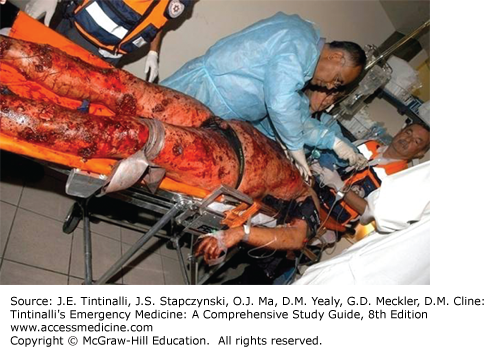
FIGURE 7-1.
Secondary blast injury to the chest and abdomen due to flying debris. It is difficult to assess the degree of underlying internal organ injury without imaging and careful clinical follow-up, especially if the patient is unconscious. [Image used with permission of Tel Aviv Medical Center.]

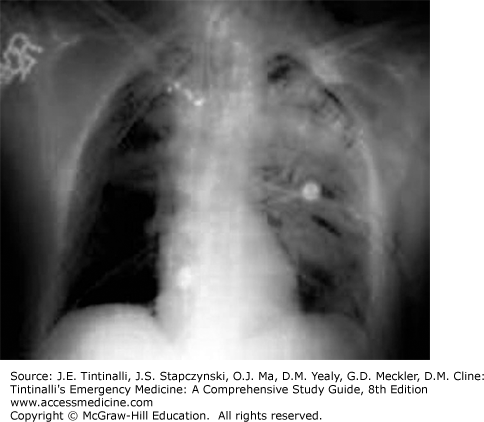
FIGURE 7-2.
This young patient came in fully conscious and hemodynamically stable. Multiple externally visible shrapnel wounds required imaging. This x-ray image shows severe lung injury due to shrapnel. She also suffered multiple abdominal injuries, including major liver lacerations and bowel perforations, and required extensive surgery. [Image used with permission of Tel Aviv Medical Center.]
The effects of a bomb blast are difficult to predict in the individual victim, as well as in the group. However, a number of important principles are known:
Distance of victim from explosion: The intensity of an explosion pressure wave declines with the cubed root of the distance from the explosion. A person 3 m (10 ft) from an explosion experiences eight times more overpressure than a person 6 m (20 ft) away. Proximity of the victim to the explosion is an important factor in a primary blast injury.
Enclosed versus open space: The effects of an explosion in a closed space, like a room, bus, or train, are much greater than in an open space. Injuries are more severe, and mortality is greater.
Surrounding environment: Blast waves are reflected by solid surfaces; thus, a person standing next to a wall may suffer increased primary blast injury.
Quantity of explosive: A greater quantity of explosive produces greater potential for damage at any distance.
Type of explosive: Explosives are commonly classified as either low-order or high-order. Low-order explosives burn rapidly and produce a blast wave of less than 1000 m/s.11 Black powder is an example of a low-order explosive. High-order explosives detonate when a shock wave passes through them, causing an almost instantaneous transformation of the original explosive material into gases occupying the same volume of space under extremely high pressure. These high-pressure gases expand rapidly, compress the surrounding medium, and produce a supersonic, overpressure blast wave, moving at greater than 4500 m/s, followed closely by a negative pressure wave.
Embedded shrapnel: Many terrorists purposefully embed multiple pieces of metal and plastic in the explosive, maximizing the number and severity of secondary injuries.
The nature of the injury may produce a multiplicity of external signs (Figure 7-3), making detection of important internal injuries challenging. Insufficient or suboptimal resources need to be prioritized in a mass casualty incident. High-grade clinical expertise is even more in demand to allow optimal use of resources.2,3,4,5,6,7,8,9
FIGURE 7-3.
The severe external injuries often seen with explosive blast may or may not indicate associated severe internal injury. Clinical examination is difficult and requires a high degree of experience and suspicion as well as early use of imaging. [Image used with permission of Tel Aviv Medical Center.]
The lung is very susceptible to primary blast injury. Pulmonary barotrauma is the most common fatal primary blast injury and the most common critical injury in people close to the blast center. Pressure differentials across the alveolar–capillary interface can cause disruption, hemorrhage, pulmonary contusion, pneumothorax, hemothorax, pneumomediastinum, and subcutaneous emphysema. Air embolism is another well-recognized consequence of blast lung injury and is probably one of the major factors leading to cardiac dysfunction and immediate death after blast wave exposure, although it is usually difficult to diagnose specifically. The resulting neurologic symptoms caused by air embolism must be differentiated from the direct effects of CNS trauma. Pulmonary fat embolism is a finding of clinical importance in survivors of blast trauma because it can lead to the development of acute respiratory distress syndrome and significantly affects clinical outcomes.
In general, managing blast lung injury is similar to caring for pulmonary contusion and acute respiratory distress syndrome, except that early recognition of the syndrome may be complicated by initially benign symptoms, especially in the context of hectic mass casualty incident situations. Hypoxia is an almost universal finding.12 Monitoring of respiratory rate and room-air pulse oximetry, as well as serial chest radiographs, may be needed. Fluid administration should ensure tissue perfusion without volume overload. The decision to institute mechanical ventilation must be made carefully because it entails the assignment of what may be scarce critical care unit beds and ventilators and also exposes the patient to the potential complications of pulmonary barotrauma, commonly seen with the friable lungs associated with blast lung syndrome. Keep tidal volume to 6 to 7 mL/kg ideal body weight to limit the peak inspiratory pressure and to minimize ventilator-induced lung barotrauma. Often, neuromuscular paralysis and early institution of pressure-limited ventilation (plateau pressures <30 cm H2O),13 with the lowest pressures compatible with adequate ventilation, may be the best strategy. Inverse inspiratory-to-expiratory ratio ventilation may be useful. Permissive hypercapnia is acceptable depending on cerebral perfusion pressure or increased intracranial pressure.13 Aggressive methods of oxygenation, such as extracorporeal membrane oxygenation or intravascular oxygenation, may become necessary within hours of the injury.
There are no definitive guidelines for observation, admission, or discharge of patients with possible blast lung injury. Admit patients requiring complex management to an intensive care unit. In general, asymptomatic patients with normal chest radiographs and normal room-air pulse oximetry may be considered for discharge after 4 to 6 hours of observation as long as there is no clinical deterioration. Survivors of this type of injury typically have no long-term pulmonary complaints, and most have normal physical examinations, chest radiographs, and normal lung function tests.
The tympanic membrane ruptures at 1 to 8 psi of dynamic overpressure. Dislodgement of ossicles may also occur. Patients with an isolated tympanic membrane perforation and no other immediately identified injuries should have a chest radiograph ordered but do not automatically require an extended period of observation. Conversely, intact tympanic membranes do not imply the absence of serious injury, and the use of the perforation of tympanic membrane as an indicator of primary blast injury missed up to 50% of those suffering a primary blast injury to the lung.14 Clinical judgment is necessary, and limited observation is reasonable for patients with intact tympanic membranes.
Abdominal injuries from explosions may be occult. Reported injury rates are low, but missed injuries may carry significant morbidity due to delayed intestinal perforation and necrosis. A review of the literature on abdominal trauma from primary blast injury reveals an incidence of 1.3% to 33%, and the terminal ileum and cecum were the most commonly injured areas.15 Serial clinical examinations, serial imaging as needed, and 24- to 48-hour observation are indicated whenever the suspicion arises. Air is a poor conductor of blast-wave energy; thus, patients who were subjected to enough energy to damage abdominal organs probably were situated near the explosive device.
The conflicts of the Global War on Terror in Iraq and Afghanistan have resulted in over a quarter of a million diagnosed cases of traumatic brain injury.16 Mild traumatic brain injury has been labeled the “signature injury of the war in Iraq.”1,17,18,19,20,21,22 The clinical examination may be misleading for penetrating injuries. Shrapnel are low-velocity missiles, often producing small entry wounds in survivors. Small entry wounds may be missed under the hair, and evidence for traumatic brain injury may initially be benign or masked by anesthesia as the patient undergoes treatment for other life-threatening injuries. Neuroimaging is an important early diagnostic tool (Figure 7-4).
FIGURE 7-4.
A. CT scan image of a 17-year-old female patient injured in a terrorist bomb blast in Israel. This girl walked into the ED unassisted, was triaged “green,” but deteriorated after 30 minutes. Fortunately the clinical deterioration was noted, she underwent emergent CT, and then extensive neurosurgical intervention. B. A 1-cm metal ball bearing was extracted. Prolonged rehabilitation was later required for residual brain damage. [Image used with permission of Tel Aviv Medical Center.]









