Chapter 107 Bites and Stings
The general principles of envenomation medicine are similar around the world, although the availability of resources varies widely. A comprehensive discussion of all available antivenins is beyond the scope of this text.1 On the basis of my experience and in consideration of space constraints, the scope of this textbook, and its audience, the chapter focuses on United States antivenins. Readers are encouraged to become familiar with the prescribing information for the antivenin(s) available in their area(s) of practice for the envenomations they may encounter.
Snakebites
Snakebite is a particularly challenging clinical problem because of the wide variety of toxic effects. Children with snakebites may have little more than a fang puncture mark, or they may have multisystem failure and death.2,3 Part of this is due to the extreme variability of snake venom, even within the same species.4 Snake venom contains multiple enzymes, proteins, and peptides that can damage local tissues and have serious systemic effects. Unfortunately, it is difficult to predict at the time of the bite which patients will have relatively mild symptoms and which will have a rapidly progressive and potentially fatal envenomation syndrome.
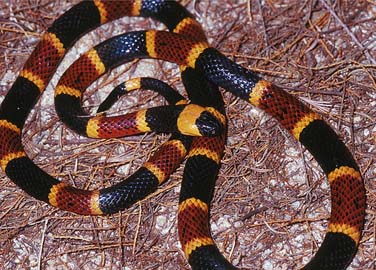
Snakebite envenomation syndromes can be loosely associated with snake family. Viperidae includes old-world vipers and pit vipers (collectively referred to as viperids). Most snakebites in the United States are inflicted by pit vipers, which include rattlesnakes, cottonmouths (also known as water moccasins), and copperheads.5 All pit vipers have a triangular head, elliptical pupils, and a heat-sensing pit between the eye and nostril (Figure 107-1).6 The pit organ has thermal receptors that can detect temperature differences of 68° C at 1.5 m in predatory interactions and 108° C at 1 m in defensive contexts (A. Krochman, personal communication, January 17, 2005). The family Elapidae (“elapids”) includes cobras, coral snakes, kraits, and mambas.7 Their venom effects can be as diverse as the species that make up this family of snakes. Cobras are showy, hooded, high-profile snakes that inhabit Africa and southern Asia (Figure 107-2). The coral snakes of the Americas and kraits of Asia and India are often small, shy, colorfully banded snakes (Figure 107-3). Mambas in Africa are long, lean, and very fast. Australian elapids can be large and nondescript. Sea snakes possess some of the world’s most toxic snake venom, although few bites occur mostly because of the marine distribution and nonaggressive temperament of these snakes. Most snakes from the Colubridae family (“colubrids”) are considered harmless, although several species possess venom and some have primitively specialized teeth to facilitate venom delivery. Some, such as the boomslang in Africa, are considered dangerous to humans, and antivenin is produced.


Epidemiology
It is often stated that children are more severely affected by snakebite than adults.8 Indeed some preliminary data suggest that smaller patients have increased severity. There is not much in terms of evidence, however, to support the assertion that outcomes for children are worse than adults. For example, of the more than 100,000 exposures and two dozen deaths described by the American Association of Poison Control Centers (AAPCC) since its first report in 1983, only a relatively small percentage of the deaths are described in pediatric patients.9 In some respects, children are no different than adults when it comes to snakebite. For instance, antivenin dosing is not based on the patient’s weight,10,11 yet there are a few concerns specific to pediatric patients. For example, because young children may not be able to give a good description of the snake or circumstances, it may be unclear whether a venomous snake has bitten them.
Pathophysiology
Although viper and pit viper venom composition varies from snake to snake, components can lead to capillary leak, abnormal clotting, inefficient muscle movement, or neurotoxicity. Capillary leak and abnormal clotting can lead to tachycardia, hypotension, or even hemorrhagic shock. Neurotoxicity or inefficient muscle movement can lead to respiratory difficulty or distress.12 Meanwhile, proteolytic enzymes, predominant in viper and pit viper venoms, digest tissue. The longer enzymatic components of venom have time to work, the more tissue gets damaged. Thus “time is tissue.”13 The sooner that antivenin can be started, the sooner that irreversible injury can be prevented.14 After tissue is injured by way of digestion, however, antivenin will not reverse the damage; it will have to heal over time.15 Myotoxicity and rhabdomyolysis can ensue.
Envenomation by most elapids is notable for severe neurological dysfunction, such as cranial nerve abnormalities, paralysis, and respiratory arrest. Some elapids, however, such as spitting and monocellate cobras, can also cause local necrosis. Most do not induce coagulopathy. Other symptoms and signs may include swelling, lethargy, vomiting, chest pain, and shock. Some cobras and cobralike species can “spit” venom toward the face of an antagonist, which can result in eye pain and visual impairment. Sea snake envenomation can cause profound neurotoxicity and myotoxicity, but generally does not induce coagulopathy or result in serious local injury. Sea snakes are found in waters around Southeast Asia and Australia. Additionally, some individuals may experience anaphylactic or anaphylactoid reactions to venom.16,17 Finally, some responses can be attributed to anxiety, although this should be a diagnosis of exclusion.6
Clinical Presentation
Immediately after a snakebite, the only apparent manifestation may be fang puncture wounds. If a patient is seen soon after a snakebite, an envenomation syndrome might not have developed yet. The onset of symptoms and signs can occur rapidly or it may be insidious. Generally the more severe an envenomation, the more rapidly it progresses; however, even a slowly progressing envenomation can lead to severe sequelae. If a patient is seen very late, the envenomation could have already run its course, and antivenin will not be as effective.14
Snakebites by pit vipers and vipers cause pain around the bite site as tissues distort with swelling. There may or may not be associated taste changes. Difficulty breathing can follow many types of venomous snakebites and can progress to respiratory distress or failure in some cases. Patients may experience nausea, vomiting or diarrhea, and venom-induced coagulopathies (often associated with viper and pit viper envenomation) can lead to hematemesis, hematochezia, or both. Certain snakebites, such as those inflicted by most elapids and some populations of rattlesnakes, can also be associated with neurological symptoms, such as motor weakness or paresthesias. Syncope or lethargy can result from severe or prolonged hypotension.6 Vital signs may reflect tachycardia, hypotension or hypertension, tachypnea, or hypoventilation. On physical examination, there may be one, two, or more fang puncture wounds, or none may be discernible. There is usually tenderness and swelling surrounding the bite site, which expands as the venom spreads locally. Other local signs can include erythema, ecchymosis, and bullae after viperid envenomation (Figure 107-4). Systemic evidence of viperid envenomation may manifest in many ways. There may be abnormal bleeding, such as prolonged bleeding from fang puncture wounds or intravenous (IV) start sites. Patients may have epistaxis or gingival bleeding. Serious and potentially life-threatening bleeding may manifest via the gastrointestinal tract or within the cranium. In extremely rare instances, snakebite can also cause hypercoagulability, which can lead to infarcts. Additionally, there may be neurological signs, such as ptosis (Figure 107-5), and muscle fasciculations or “myokymia.”6

Figure 107–4 Southern Pacific rattlesnake (Crotalus helleri) bite wounds.
(Photo Courtesy Sean Bush, MD.)

Diagnostic Studies
Initial laboratory tests after pit viper or viper envenomation should include a complete blood count (CBC), prothrombin time (PT), partial thromboplastin time (PTT), international normalized ratio (INR), fibrinogen, and a type and screen. Venom-induced coagulopathy is common after many types of viperid envenomations and is most typically characterized by thrombocytopenia and hypofibrinogenemia. Even if coagulation values are normal on presentation, they may need to be rechecked depending on the clinical scenario. Venom-induced coagulopathies can develop late, recur, or persist. If initial laboratory findings are abnormal, more frequent monitoring may be necessary depending on how severely abnormal they are and how they respond to treatment. If the findings are abnormal, repeating the CBC, PT, PTT, INR, and fibrinogen tests 1 hour after completion of an infusion of antivenin may be helpful to monitor treatment efficacy. When laboratory values are rechecked, in addition to the initial laboratory panel, additional blood should be sent for creatine kinase (CK), electrolytes, blood urea nitrogen, and creatinine clearance. All snakebite can result in rhabdomyolysis, which usually responds to aggressive fluid hydration, but can require dialysis if myoglobinuric renal failure develops. In certain regions, such as Australia, venom detection kits (e.g., enzyme-linked immunosorbent assays) may be available to help identify species and guide specific antivenin selection. Other diagnostic studies may be indicated on the basis of a patient’s medical history or special circumstances.6
Prehospital Care
The factors that most reduce snakebite-related injury and death in the United States are rapid transport, intensive care, and the administration of antivenin.18 All patients with snakebites should be transported to the hospital as expeditiously and safely as possible, preferably through a 911 call (where available). The following measures are not recommended for first aid: incision, suction, tourniquets, electric shock, ice directly on wound, alcohol, or folk therapies.19–21 Insufficient evidence exists for splinting or positioning (e.g., above or below the level of the heart). Therefore the extremity should initially be maintained in a neutral position of comfort. The Australian technique of pressure immobilization resulted in significantly longer survival, but higher intracompartmental pressures after artificial, intramuscular (IM) western diamondback rattlesnake envenomation in a pig model.22 This technique involves immediately wrapping the entire extremity that was bitten starting at the bite site and proceeding proximally with an elastic Ace wrap or crepe bandage as tightly as one would wrap for a sprain, then splinting and immobilizing the extremity. Although pressure immobilization is not recommended widely, certain scenarios may warrant its use. It is generally not recommended for most viper bites or for bites by spitting cobras, but it is recommended for most types of Australian fauna, cape cobras, kraits, coral snakes, mambas, and sea snakes. Once pressure immobilization is placed, it should not be removed until preparations are made to manage acute toxicity and/or immediate hypersensitivity because of a potential bolus effect after its removal. Although it is difficult to predict snakebite severity at the time of the bite, certain factors may reflect increased likelihood of a more severe envenomation: large snake size, dangerous snake species, small patient size, prolonged fang contact, previous snakebites (treated or not) or exposures to snakes, or delays to medical care.
Emergency and Critical Care
All emergency personnel should be able to distinguish a venomous from a nonvenomous snake if it occurs naturally in their region of practice. If there is uncertainty about whether a particular snake is venomous, consider taking photographs of the snake from a safe distance of at least 6 feet away using a digital or Polaroid camera. These images can be seen immediately and may help make clinical decisions. Although it may be helpful to identify the species of snake,15,23 transporting it (alive or dead) is discouraged because of inherent dangers with capturing it. On scene, snakes should only be moved or contained if absolutely necessary. A snake hook or long shovel may be helpful to move the snake into a large, empty trash canister where it can be recovered by professionals, such as an animal control agent.
All hospitals should stock at least enough antivenin to treat one patient. This should be arranged ahead of time if possible, although sometimes there are antivenin shortages and other resource challenges. Presently only one agent is commercially available in the United States for treatment of pit viper envenomation: Crotalidae Polyvalent Immune Fab (Ovine), which goes by the trade name CroFab (Protherics Inc., Nashville, Tenn.).24 Antivenin Crotalidae Polyvalent is no longer produced. Several manufacturers produce antivenin for bites in Africa (e.g., South African Vaccine Producers), Asia, Europe, and Australia (e.g., Commonwealth Serum Laboratories [CSL]), and the Americas (e.g., Instituto Bioclon in Mexico, Instituto Clodomiro Picado in Costa Rica, and the Butantan Institute in Brazil). A polyvalent sea snake antivenin (CSL) is the drug of choice for sea snake envenomation, but tiger snake antivenin may have adequate efficacy if sea snake antivenin is not available. Information on antivenin should be researched ahead of time, and practitioners should be familiar with sources and administration techniques for the antivenins available for envenomations they may encounter. Each antivenin has varying specificity, efficacy, and safety. Some antivenins developed for one species may have some efficacy against other closely related species. If an exotic envenomation is encountered in the United States, calling the AAPCC or consulting the Antivenom Index may help locate antivenin. Many zoos stock antivenins for the exotic species they keep. If antivenin is unavailable, a patient with an elapid or sea snake envenomation may need his or her airway secured and ventilatory support provided for days or even weeks. Meanwhile, hypotension should be treated with IV fluids and then vasopressors. Edrophonium may temporarily improve weakened muscles of respiration after elapid envenomation while awaiting antivenin.
There are various suggested methods to determine the need for antivenin in your patient. Many grading scales are available, but it is better to treat a patient based on envenomation progression or potential. Grading scales should not be used for elapid or sea snake envenomations. Antivenin should be given promptly for best results, although it may have benefit for days to weeks after an envenomation. Anytime antivenin is given, allergic reactions should be anticipated. It may be helpful to know whether the patient has allergies or previous exposures to papain, papaya or animal serums, or other agents used to make antivenin. Obtain informed consent when possible. Many of the principles of antivenin administration are similar. The technique for administering CroFab is outlined as an example. A starting dose of CroFab is 4 to 6 vials,25 which is the same for children as it is in adults. Each vial is reconstituted with 10 ml of sterile water. It can take anywhere from about 10 to 30 minutes to go into solution. It is best to swirl or roll the vials between the hands rather than to shake them. After each vial goes into solution, it should be further diluted into a total volume of 250 mL of normal saline. No skin test is recommended for CroFab, although manufacturers of many other types of antivenin recommend skin testing. With CroFab, the infusion is started slowly, at a rate of 1 mL/min for the first 10 minutes. While the infusion is started, a physician skilled in resuscitation should be at bedside. Difficult airway equipment, epinephrine, diphenhydramine and a histamine (H2) blocker (e.g., cimetidine) should be immediately available. If the infusion is tolerated for the first 10 minutes without evidence of an adverse reaction, the rate should be increased to complete thee total volume of 250 mL/hour. If there is a problem at any time, stop the infusion, treat the adverse reaction accordingly, and reassess the need to continue antivenin treatment. A physician should be nearby at all times during the remainder of the infusions. Repeat four- to six-vial increments until initial control is achieved. Initial control is defined as the arrest or significant slowing of progression of any and all components of the envenomation syndrome (i.e., minimal to no further advancement of swelling, improvement of systemic effects, and improving coagulopathy). Assess at up to 1 hour after each dose. After initial control is achieved, a maintenance dose of two vials of CroFab every 6 hours for three doses is recommended in the prescribing information, although maintenance dosing has been shown not to reduce recurrence phenomena.26 Read the package insert for additional details.25 For pharmacokinetic reasons that are not entirely understood, recurrence phenomena are associated with antivenins.27–29 Local recurrence is the return of new progressive swelling after initial control. That is, the leading edge of tenderness or swelling begins to advance again. An additional two vials of CroFab should be given as soon as progressive swelling recurs, and more antivenin may be necessary to regain control, although experience has shown that local effects may continue to progress despite additional antivenin. Patients with rattlesnake bites commonly have thrombocytopenia and hypofibrinogenemia, which can resolve with CroFab and then recur (coagulopathy recurrence). Indications for an additional two vials of CroFab are serious abnormal bleeding, fibrinogen less than 50 μg/mL, platelet count less than 25,000 mm3, INR greater than 3, multicomponent coagulopathy, worsening trend in patient with prior severe coagulopathy, high-risk behavior for trauma, or comorbid conditions that increase bleeding risk. Coagulopathy can recur as late as 2 weeks or more after treatment.
Prophylactic antibiotics are unnecessary. Empiric antibiotic therapy should only be started if an infection develops and once aerobic and anaerobic wound cultures have been obtained. If an abscess occurs, it should be drained in standard fashion. An infected snakebite should prompt a further examination of the wounds for potential retained teeth or fangs.5
Envenomations by vipers and pit vipers are remarkable for the amount of swelling they can produce. With prompt and adequate antivenin treatment, fasciotomy or digit dermotomy is rarely indicated, even after severe viperid envenomation.30–33 Fasciotomy, however, may be indicated if measured compartment pressures remain persistently and severely elevated despite adequate antivenin. Antivenin has been shown to limit the decrease in perfusion pressure associated with compartment syndrome.34 Compartment syndrome may manifest subjectively, with complaints of increasing pain, and objectively, with tenderness on passive muscle stretch, a rock hard feel to the compartment, or a diminished capillary refill. True compartment syndrome, however, is rare after snakebites, even in patients with severe swelling. It may be difficult to distinguish compartment syndrome from the effects of envenomation. Similar to compartment syndrome, viperid envenomation may cause a bluish discoloration of the skin or pallor (because of subcutaneous bruising), severe swelling, paresthesias, and pain. If effects are only caused by envenomation and the patient does not have compartment syndrome, capillary refill should be normal and compartmental pressures should not be elevated. If compartment pressures are elevated, Gold et al.31 recommend limb elevation, along with IV mannitol (1 to 2 mg/kg) administration and an additional four to six vials of CroFab over 1 hour. Consultation with a surgeon (e.g., general, orthopedic, or hand) should be initiated concurrently. Compartment pressures should be measured before surgical intervention.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


