Chapter 39 Assessment and Monitoring of Respiratory Function
The majority of children admitted to the pediatric intensive care unit (PICU) present with cardiorespiratory disease or with an acute illness that may progress to involve the respiratory system, emphasizing the need for careful monitoring of respiratory parameters. Close respiratory examination and monitoring allow titration of therapies to minimize ventilator-induced injury, optimize patient-ventilator interaction, and aid in weaning from the ventilator.1
Physical Examination of the Respiratory System
Evaluation of breath sounds provides assessment of airflow through the tracheobronchial tree, the presence of fluid in or obstruction of the airways, and conditions outside the lung and pleural space. The child’s chest wall is thinner than that of the adult, which allows better access to breath sounds but impedes localization of the lesion because the breath sounds can be referred. Upper airway abnormalities may present with stridor or muffling of the voice. Bronchial breath sounds suggest consolidation, whereas wheezes result from narrowed airways. Crackles may be fine or coarse. They represent air bubbling through secretions and the reopening of closed airways. A friction rub may be heard when the inflamed surfaces of the pleura move against each other through the respiratory cycle. Breath sounds may be absent if there is a significant pleural effusion or complete lobar collapse resulting from a mucus plug or pneumothorax. Heart tones often are shifted away from the pneumothorax and toward the atelectasis because of complete airway obstruction. Assessment for pulsus paradoxus (i.e., exaggerated decrease in the pulse or systolic blood pressure with inspiration) should be made during the evaluation of severe airway obstruction or pulmonary embolus.
Although each assessment should include observation and a limited physical examination, it is recognized that interobserver repeatability of physical signs is poor and independent of the experience of the observer.2 The assessments of clubbing, wheezes, friction rub, and crackles are the most reliable and reproducible.2,3 The lack of accuracy of repeated physical examinations and the complexity of critically ill pediatric patients require adjunctive tests/assessments to monitor these patients.
Radiography
Portable chest x-ray films are the most common films taken in the PICU. The technical quality of the chest radiograph affects the interpretation; therefore, it is important to assess the film for adequacy of penetration, degree and symmetry of lung inflation, and degree of chest rotation. Chest x-ray films can be used to evaluate for cardiac, vascular, bone, and lung abnormalities, to assess for device placement (e.g., an endotracheal tube), and to determine the need for intervention.4 Lateral decubitus films help identify and quantify pleural effusions, pneumothorax, and the position of chest tubes/lines. Cross-table lateral films also may be used for these purposes but are harder to interpret. A chest computed tomography (CT) scan is used when details on the plain film are obscured by the superimposition of structures or an opaque hemithorax. A chest CT scan also can be used to guide drainage of fluid collections and assist in obtaining biopsy specimens. A high-resolution chest CT scan examines 1- to 1.5-mm slices at 10-mm intervals; therefore it can be used to illustrate lung parenchymal details better than a conventional CT scan, which examines 7- to 10-mm slices at 10-mm intervals.5 This detail can be helpful in distinguishing the pathologic process causing diffuse lung diseases that appear as diffuse lung shadowing on chest x-ray films. Chest ultrasound, ventilation/perfusion scanning, spiral CT, and magnetic resonance imaging may be useful adjutants depending on the disease process.
Noninvasive Respiratory Monitoring
Pulse Oximetry
Pulse oximetry is considered a significant technologic advance that has improved patient safety.1,6–9 Its ease of application and accuracy have resulted in widespread use. Pulse oximetry is commonly used to detect hypoxemia and to wean the oxygen concentration in patients undergoing mechanical ventilation.
Pulse oximetry is based on the principles that (1) the pulsatile absorbance detected is arterial blood and (2) oxyhemoglobin and reduced hemoglobin have different absorption spectra.6 Red (660-nm) and infrared (940-nm) wavelengths of light are used to determine the ratio of oxygenated to deoxygenated blood. Deoxygenated blood absorbs more red light, whereas oxygenated blood absorbs more infrared light. The two wavelengths are passed through an arterial bed, and the ratio of infrared and red light transmitted to the photodetector is determined. The ratio is calibrated against measurements of arterial oxygen saturations from human volunteers and their absorbance ratios.
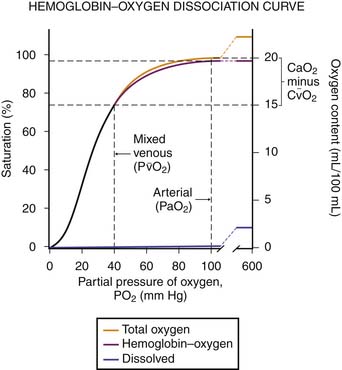
Several factors may affect the accuracy of pulse oximetry. Pulse oximetry measures oxygen saturation (SaO2). SaO2 and PaO2 are not linearly related; the oxyhemoglobin dissociation curve is sigmoid in shape (Figure 39-1). Large changes in PaO2 at high levels of oxygen, the upper flat portion of the oxyhemoglobin dissociation curve, may occur with little change in saturation. Additionally, a reduction in oxygenation on the steep portion of the curve may not be appreciated as significant because only a small change in saturations will have occurred.6,7 The accuracy of pulse oximetry falls with arterial oxygen saturations less than 70%.1,6 At arterial oxygen saturations below 70%, pulse oximetry may be more appropriate for showing trends.6
< div class='tao-gold-member'>





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


