90 Arterial and Venous Trauma and Great Vessel Injuries
 Key Points
Key Points• Thirty percent of patients with great vessel injury (GVI) die within 6 hours of hospital arrival.
• Thirty percent to 50% of patients with blunt aortic injury have no signs of trauma.
• A normal chest radiograph does not exclude GVI.
• Computed tomographic angiography is the diagnostic test of choice to rule out traumatic aortic injury in hemodynamically stable patients.
• For patients too large for a computed tomography scanner, transesophageal echocardiographic evaluation of the aorta should be considered.
• Medical management of GVI is typically used as a bridge to more definitive operative care.
• β-Adrenergic blockade is instituted before nitroprusside in the medical management of GVI to avoid possible reflex tachycardia.
Epidemiology
Few traumatic injuries are more devastating than great vessel injury (GVI). With an average circulating volume of 5 L and a flow rate of up to 4.8 L/min in the circulatory system, it is easy to see why GVI can result in catastrophic outcomes quickly. The true incidence of traumatic aortic injury may never be known; however, according to the National Trauma Data Bank, blunt thoracic aortic injury occurred in 0.3% of trauma patients admitted to the hospital during a 5-year period.1 When patients survive an initial injury to their great vessels, rapid diagnosis and treatment are imperative to prevent subsequent exsanguination within the next minutes to hours. This highlights the ever-emphasized “golden hour” of trauma resuscitation.
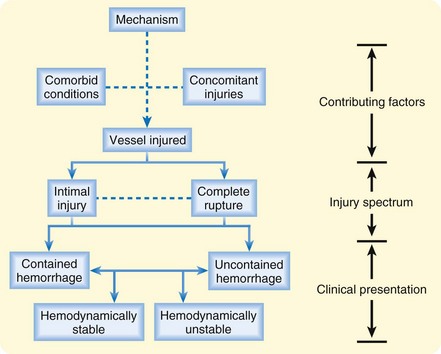
Several contributing factors are important when evaluating potential GVI (Fig. 90.1). Although the mechanism and specific vessel injured are the most important of these factors, significant attention must be paid to the role of concomitant injuries and comorbid conditions on patients’ morbidity and mortality. Unfortunately, on initial evaluation the emergency physician is often lucky to be privy to one, let alone all, of these factors.
The most important branch point for both the likelihood and the type of GVI is a penetrating versus blunt mechanism. Penetrating mechanisms are associated with greater than 90% of great vessel trauma, and any thoracic vascular structure is at risk.2 Patients who survive to arrive at the emergency department, particularly if they are not in hemorrhagic shock, have a survival rate that approaches 50%.3
In contrast, blunt traumatic injuries to the great vessels most often affect the aorta, although the innominate artery, pulmonary hilar vessels, and vena cava are also susceptible. Blunt aortic rupture carries an immediate mortality rate of greater than 80% and is responsible for 10% to 15% of motor vehicle accident fatalities.4 Because of the high association of blunt ascending aortic injury with fatal cardiac injury, the vast majority of those who survive to hospital evaluation have descending injuries. Of patients who survive until medical evaluation, 30% die within 6 hours and 40% within 24 hours.4 Because most of these injuries occur in young healthy males, the overall survival rate is much better than expected given the severity of injury.
Though incompletely understood, it is proposed that blunt aortic injury can result from any combination of shearing forces, rotational forces, increased intraluminal aortic pressure, or a pinching mechanism between the sternum and vertebral column. Given these forces, it is not a surprise that motor vehicle collisions cause the majority of blunt aortic injuries. This association increases with the speed of the accident.5,6 Shearing forces were originally thought to be the highest in frontal-impact accidents, where deceleration forces are the greatest. More recent studies, however, have shown that side-impact accidents are associated with a higher risk for blunt aortic injury. A review of 119 cases of known blunt aortic injury as a result of car accidents in the United Kingdom found that lateral impact direction to the same side was highly associated with aortic injury.7 A review of accident data from the United Kingdom and United States in 2004 mirrored these results and found that side impact involving the patient’s side of the vehicle carried a significantly higher risk for aortic injury than did frontal impact.8 Although motor vehicle accidents account for the majority of blunt GVI, falls from a height and crushing forces have also been known to cause the disease process.5
In part because of difficulty isolating the hilum, injuries to the pulmonary arteries, veins, and thoracic vena cava are associated with mortality rates greater than 60%, regardless of whether they are caused by blunt or penetrating force, although the latter is much more common.9
Concomitant injuries clearly play a role in the epidemiology, morbidity, and mortality of GVI. One study on blunt thoracic trauma showed that patient with traumatic aortic injury carried a mean injury severity score (ISS) of 40 whereas patients without vascular injury had a mean ISS of just 16.5 Another showed that closed head injury was diagnosed in more than half of patients with GVI, with one quarter having intracranial hemorrhage.3
PathopHysiology
Arterial System
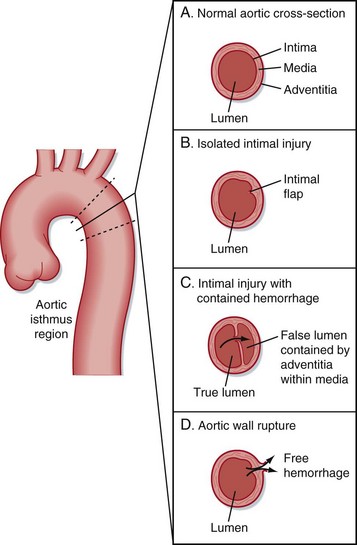
The microanatomy of the artery wall, with its intimal, medial, and adventitial layers, is integral in the spectrum of disease. Injuries range from isolated thrombogenic intimal flaps to full-thickness tears with free hemorrhage (Fig. 90.2).
Presenting Signs and Symptoms (Box 90.1)
Traditionally, aortic dissection as a result of nontraumatic causes is believed to be manifested as tearing pain radiating through the chest to the interscapular region of the back. This pain can be accompanied by various degrees of associated symptoms, including shortness of breath or vagal complaints. In patients with traumatic injury, this symptom pattern is seen less than 25% of the time; these patients most frequently either have vague chest-related complaints or no complaints at all because of distracting injuries. A remarkable 30% to 50% of patients with a blunt aortic injury may have no external signs of trauma.10




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


