191 Approach to the Adult Rash
 Key Points
Key Points• Rashes are a common reason for a visit to the emergency department. Some rashes are simple and straightforward. However, others represent the initial complaint of a patient with a life-threatening disease.
• Fever with a rash is key to recognizing some of the more dangerous conditions.
• The key for differentiating a diffusely erythematous rash includes the presence or absence of the Nikolsky sign.
• Key factors for differentiating a maculopapular rash include its distribution and target lesions.
• A vesiculobullous rash is also differentiated by distribution; a localized or diffuse distribution helps narrow the differential diagnosis.
• Petechial/purpuric rashes are differentiated by the presence or absence of palpable lesions.
• Petechiae do not blanch with pressure.
• Palpable purpura occurs in vasculitic diseases secondary to inflammation or infection.
• Nonpalpable purpura is characteristic of thrombocytopenic conditions.
• Bullous rash with mucosal involvement is worrisome, and steroid therapy may be warranted.
• A careful history and physical examination are crucial for narrowing the differential diagnosis of an unknown rash.
Epidemiology
Evaluation of rashes ranks highly among the top 20 reasons for visits to the emergency department.
A well-reasoned algorithmic approach to the evaluation of rashes might aid the emergency medicine specialist in identifying the most common and potentially lethal rash syndromes. Although an exhaustive review of all potential fungal, parasitic, and viral causes of rash is beyond the scope of this chapter, the algorithms presented will equip physicians to quickly recognize the most common and critical rashes. Pediatric rashes are discussed in detail in Chapter 18. Additionally, the most life-threatening rashes are discussed in more detail in Chapter 192.
Pathophysiology
A rash is a skin eruption that has a defined morphology and location. The morphology of the rash is usually distinct and related to the pathophysiologic dysfunction of the skin. Most severe rashes begin as exanthems (from the Greek exanthema, which means “breaking out,” and anthos, which means “flowering”). These rashes subsequently take on a particular morphology, characteristic lesions, or distribution. Table 191.1 delineates the most common terms used for skin lesions. Understanding these terms helps one better document progression of disease and facilitates communication with consulting physicians.
Table 191.1 Common Terms for Skin Lesions
| TERM | DESCRIPTION |
|---|---|
| Lesion | Single small diseased area |
| Macule | Circumscribed area of change without elevation |
| Rash | Skin eruption that is more extensive than a single lesion |
| Papule | Solid raised lesion < 1 cm |
| Nodule | Solid raised lesion > 1 cm |
| Plaque | Raised confluence of papules > 1 cm |
| Pustule | Fluid-filled area containing purulence |
| Vesicle | Fluid-filled area < 1 cm containing clear fluid |
| Bullae | Fluid-filled area > 1 cm |
| Petechiae | Pinpoint flat round spots < 3 mm caused by intradermal bleeding that do not blanch |
| Purpura | Hemorrhagic area > 3 mm that does not blanch |
| Exanthem | Rash outside the body (skin) |
| Enanthem | Rash inside the body (mucous membranes) |
Presenting Signs and Symptoms
Eliciting the initial distribution and progression of a rash is essential. Additionally, the involvement of palms, soles, and mucous membrane is of key importance. It should be kept in mind that dysphasia, as well as eye or genital irritation, may be a manifestation of as mucosal involvement and is often the initial symptom of several life-threatening conditions. The rash’s rapidity of progression is also an essential in diagnosis. Box 191.1 categorizes these important findings.
Box 191.1 Distribution and Progression of a Rash
Specific Signs
Two signs are important in the evaluation of these rashes: the Nikolsky sign and the Asboe-Hansen sign. A positive Nikolsky sign (Fig. 191.1) is noted when slight rubbing of the skin results in exfoliation of the outermost layer with lateral extension of the erosion into the intact skin. The area of denuded skin is pink and tender. The Asboe-Hansen sign (indirect Nikolsky sign or Nikolsky II sign) is extension of a blister into normal skin with the application of light pressure on the top of the blister. All patients with tender, blistering, or sloughing skin should be evaluated serially for these important signs.

Differential Diagnoses and Medical Decision Making
The Algorithmic Approach
Erythematous Rashes
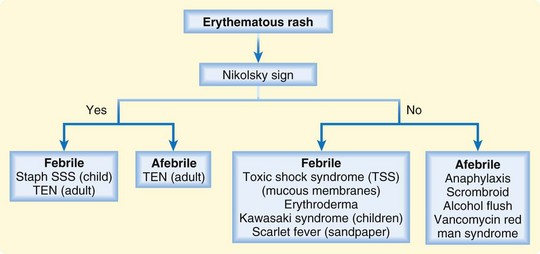
These rashes are characterized by diffuse redness of the skin as a result of capillary congestion. Erythematous rashes are differentiated by the presence or absence of fever and the Nikolsky sign (Fig. 191.2).1 If a Nikolsky sign is present, the diagnosis is narrowed substantially, usually to TEN in adults and to staphylococcal scalded skin syndrome (SSSS), generally in infants and young children. If fever is present without a Nikolsky sign, the differential diagnosis includes Kawasaki disease, scarlet fever, erythroderma, and toxic shock syndrome (TSS). Patients with an erythematous rash but without a fever or Nikolsky sign may be having an anaphylactic reaction or a reaction to vancomycin, scombroid, or alcohol exposure. Please refer to Chapter 18 for review of SSSS, Kawasaki disease, and scarlet fever. Refer to Chapter 192 for review of TEN, TSS, and erythroderma.
Maculopapular Rashes
The term maculopapule is a portmanteau of macule and papule. Maculopapular rashes are differentiated by the distribution of the rash and systemic toxicity (Fig. 191.3). Patients with centrally distributed rashes who appear toxic and febrile have a wide differential diagnosis; however, it is paramount that patients living in endemic areas be assessed for Lyme disease. Those with centrally distributed rashes but no signs of toxicity usually have either a drug reaction or pityriasis rosea. Patients with peripherally distributed rashes have a broader differential diagnosis that is dependent on systemic toxicity, the presence or absence of target lesions, and whether the rash is located on the flexor or extensor surfaces. Target lesions (Fig. 191.4) are pathognomonic for SJS or erythema multiforme (EM). The target lesion of Lyme disease is usually a single large bull’s eye that measures at least 5 cm in diameter (erythema migrans). Patients with peripheral lesions and systemic toxicity but without target lesions require emergency evaluation for meningococcemia, RMSF, and syphilis. Nontoxic patients with a peripherally distributed rash and no target lesions require further assessment for flexor involvement (scabies or eczema) or extensor involvement (psoriasis). Please refer to Table 191.2 for review of EM minor and major. See Chapter 18 for review of viral exanthems. Please refer to Chapter 192 for review of Lyme disease, meningococcemia, RMSF, SJS, and syphilis.
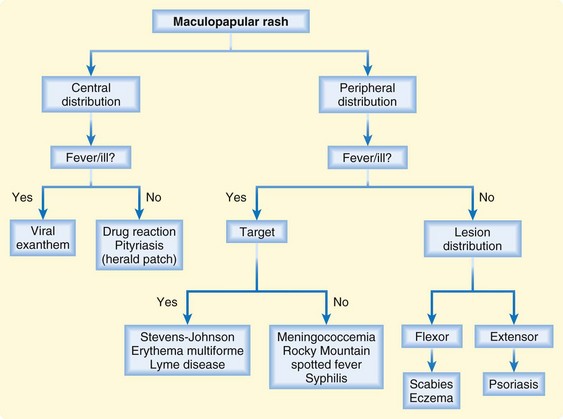
Fig. 191.3 Algorithm for maculopapular rashes.
(From Murphy-Lavoie H, LeGros TL. Emergent diagnosis of the unknown rash: an algorithmic approach. Emerg Med 2010;42[3]:6-17.)



Table 191.2 Erythema Multiforme
| Causes | Possibly autoimmune | |
| Unknown in 50% | ||
| Exposures | Infections: herpes simplex, Mycoplasma, fungi | |
| Drug exposures: sulfa and other antibiotics, anticonvulsants | ||
| Classification | Erythema multiforme minor | Erythema multiforme major |
| Description | Mild, self-limited rash | |







