65 Aortic Dissection
 Key Points
Key Points• Aortic dissection is deadly and difficult to diagnose. It is suspected less than half the time at initial evaluation.
• Ninety percent of patients with aortic dissection have sudden, severe, or unrelenting pain in the chest or upper part of the back, or in both areas.
• When a patient has chest pain with a pulse deficit or any acute neurologic deficit, aortic dissection is the most likely diagnosis.
• D-dimer is a sensitive biomarker for ruling out dissection. Computed tomographic angiography is the study of choice for making the diagnosis.
• Systolic blood pressure in patients with aortic dissection should be maintained at less than 120 mm Hg regardless of the patient’s baseline blood pressure unless symptoms or signs of organ malperfusion are present. Beta-blockers are the first-line antihypertensives.
Epidemiology
A patient in the emergency department (ED) whose proximal aorta has dissected has about a 2% chance of dying every hour during the first 12 hours and almost a 50% chance of dying within 48 hours without surgical treatment.1,2 Unfortunately, this disease is often difficult to diagnose. A study involving three academic EDs found that the diagnosis was suspected during the initial encounter in only 43% of cases.3
The incidence is 3 per 100,000 people per year.4,5 A typical large urban ED sees several cases per year.3 About 1 in 350 patients evaluated in an ED for chest pain has aortic dissection.4–6
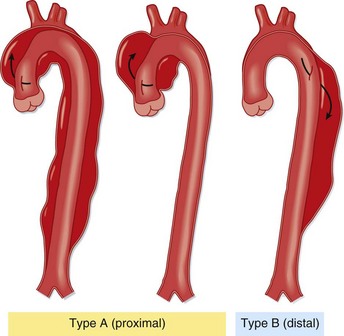
Sixty percent of aortic dissections involve the ascending aorta, either alone or with other parts of the aorta; they are referred to as type A in the now standard Stanford classification. The 40% that do not involve the ascending aorta are Stanford type B (Fig. 65.1). This distinction has important prognostic and therapeutic implications.
The Young Patient
About 7% of patients with aortic dissection are young (<40 years) and usually have no history of hypertension or other known medical problems.7 These patients nearly always have occult structural cardiovascular disease.
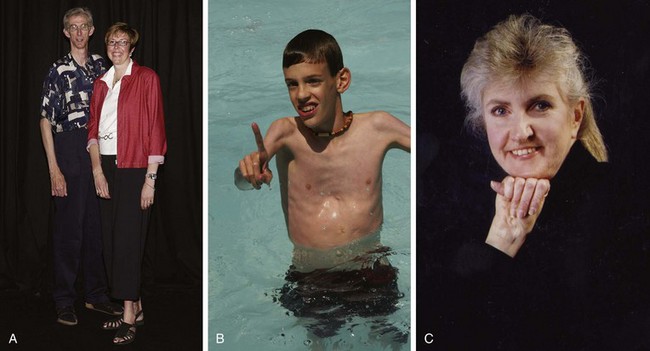
The most important structural vascular disease is Marfan syndrome, which has a prevalence of 1 in 10,000 and occurs in all races. Marfan syndrome accounts for half of aortic dissections in patients younger than 40 years.7 It is caused by an autosomal dominant mutation in the gene for a type of fibrillin, a protein that makes up part of the elastic fibers in connective tissue of the aorta, lens, and periosteum. Patients are typically tall with long digits, scoliosis, pectus excavatum, and visual problems because of lens dislocation (Fig. 65.2, A to C). Most important, however, thoracic aneurysms invariably develop early in life, usually in the ascending aorta. If their aneurysms are not repaired, most patients will die of aortic dissection or rupture.
Other young patients without a history of severe hypertension who are nevertheless at risk for dissection are those with bicuspid aortic valves and those experiencing acute insults such as cocaine use and trauma. A family history of aortic aneurysms and dissection, beyond syndromes usually associated with aortic pathology, is a newly recognized risk factor seen in 10% to 20% of patients with dissection.8
Pathophysiology
The aorta dissects by two possible mechanisms (Fig. 65.3). The classic mechanism is an intimal tear, which is generally transverse and extends through the very thin tunica intima into the tunica media. Under pulsatile force, blood enters a layer of the media and dissects longitudinally and usually in a distal direction. The other major mechanism is rupture of the vasa vasorum, usually of a penetrating branch within the tunica media, with consequent bleeding into the media. Progression then occurs in the same fashion, either with or without secondary tearing through the intima into the aortic lumen. The aorta generally tears near tethering points, where the vessel undergoes the greatest flexion stress during cardiac contractions. Thus the most common location for initiation of dissection is the first few centimeters of the ascending aorta, the next most common being the origin of the descending aorta just distal to the left subclavian artery.
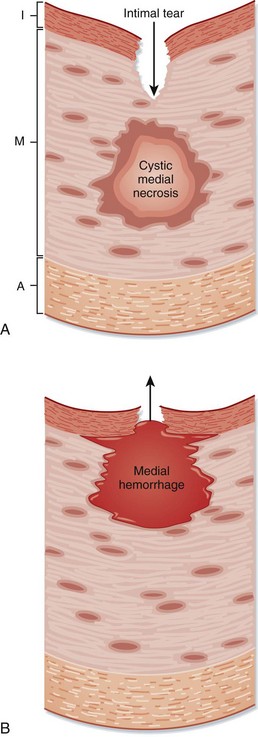
Fig. 65.3 Two mechanisms of aortic dissection.
A, Intimal tear. B, Rupture of the vasa vasorum. A, Adventitia; I, intima; M, media.
(From Zipes DP, Libby P, Bonow RO, et al, editors. Braunwald’s heart disease: a textbook of cardiovascular medicine. 7th ed. Philadelphia: Saunders; 2005.)
Those who suffer dissection are predisposed to it by a weakened aorta, specifically, degeneration of the tunica media, or suffer a hemodynamic or traumatic insult, or both (Table 65.1).7–9 Medial degeneration can be secondary to chronic hypertension, hereditary diseases of elastin (Marfan syndrome) or collagen (Ehlers-Danlos syndrome), hereditary structural abnormalities (bicuspid aortic valve and aortic coarctation), chronic inflammation, and aneurysm of any cause, which increases wall tension according to Laplace’s law.
Table 65.1 Risk Factors for Aortic Dissection
| RISK FACTORS | PREVALENCE (%) |
|---|---|
| Common Factors | |
| Hypertension | 70 |
| Family history of aortic dissection or aneurysm | 10-20 |
| Aortic aneurysm (known) | 13 |
| Previous aortic dissection | 5 |
| Marfan syndrome | 5 (50% in patients < 40 yr) |
| Aortic valve disease: atrioventricular replacement, bicuspid aortic valve | 9 |
| Iatrogenic: cardiac surgery, cardiac catheterization | 4 |
| Uncommon Factors | |
| Cocaine or methamphetamine use | |
| Pregnancy | |
| Weight lifting | |
| Ehlers-Danlos syndrome—vascular type | |
| Coarctation of the aorta | |
| Chronic inflammation | |
| Giant cell (temporal) arteritis | |
| Takayasu arteritis | |
| Tertiary syphilis | |
| Trauma | |
Presenting Signs and Symptoms
Dissection of the aorta is usually extremely painful, so acute pain is a chief complaint in nearly 95% of cases (Table 65.2).7,10–14 Aortic pain is sudden and maximal at onset, with its intensity often proportional to the length of dissection. The location of pain is midline and, classically, correlates with the location of dissection: dissection of the ascending aorta results in chest pain, dissection of the arch results in neck or jaw pain, and dissection of the descending aorta results in back and sometimes abdominal pain. Thus the pain may migrate as the dissection propagates. However, there is considerable variability in symptoms and major overlapping of symptoms in type A and type B dissections.3,9
Table 65.2 Symptoms, Signs, and Findings in Patients with Aortic Dissection
| PREVALENCE (%) | |
|---|---|
| History | |
| Pain | |
| Any | 94 |
| Sudden | 90 |
| Severe | 90 |
| Migrating | 25 |
| Tearing/ripping | ≈35 |
| Chest pain | 67 |
| Back pain | 50 |
| Abdominal pain | 25 |
| Syncope | 12 |
| Physical Findings | |
| High blood pressure | 50 |
| Hypotension or shock | 15 |
| Diastolic murmur | 33 |
| Pulse deficit | 30 |
| Focal neurologic deficit | 15 |
| Study Results | |







