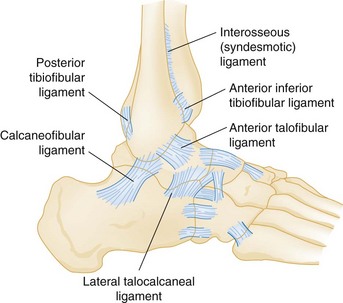
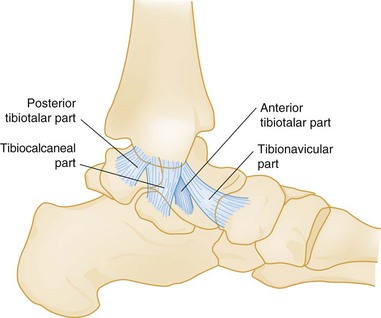
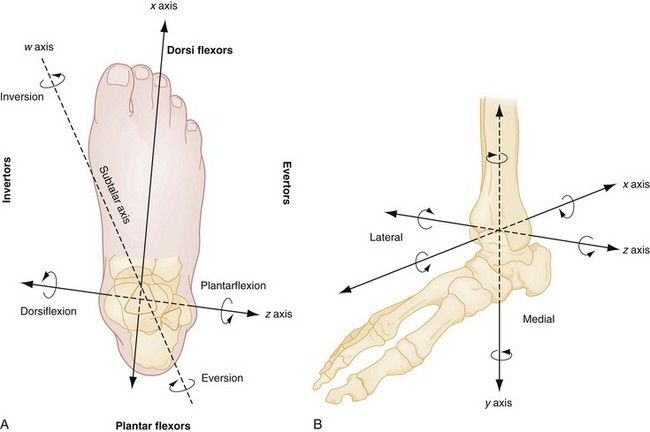
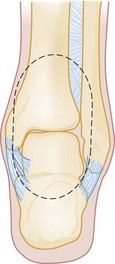
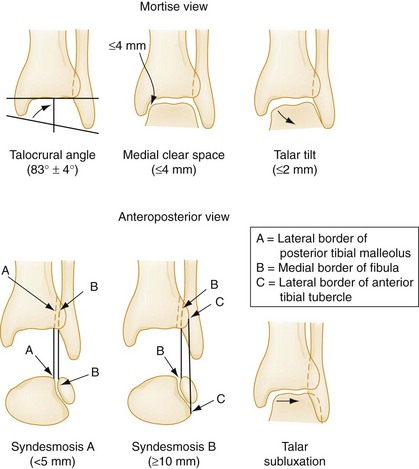
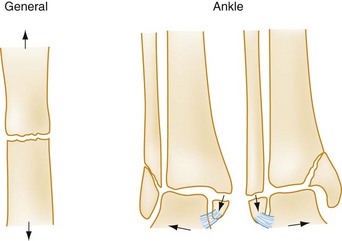
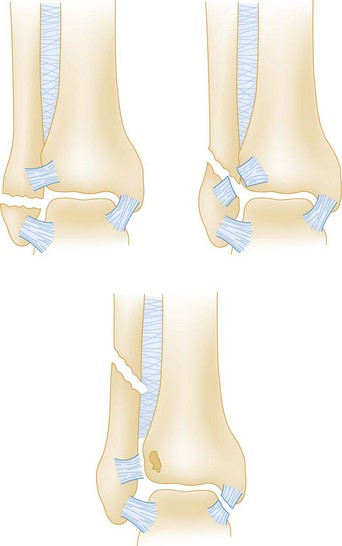
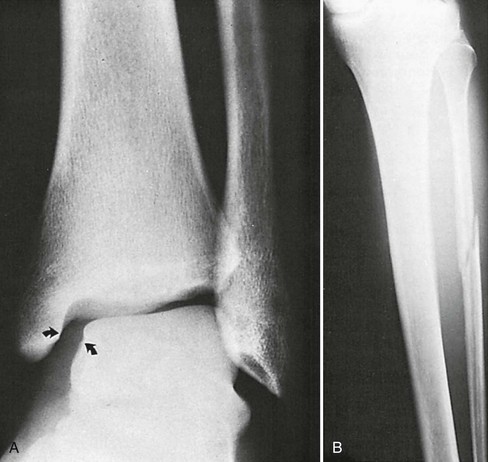
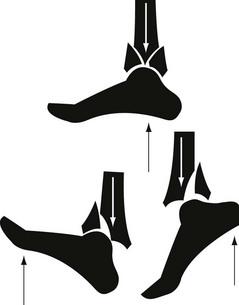
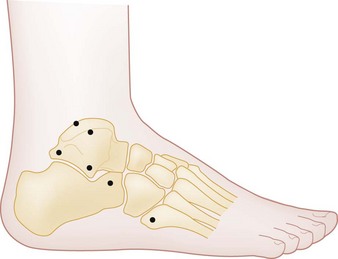
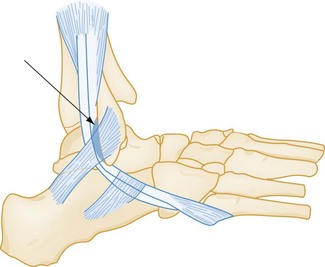
Chapter 58 Three sets of ligaments—the syndesmotic ligaments, the lateral collateral ligaments, and the medial collateral ligaments—support the ankle joint and are essential to its stability (Figs. 58-1 and 58-2). Ankle movements are complex and often involve more than one joint. It is best to consider the group of joints about the ankle as one unit, the ankle joint complex. This complex, which is made up of the talocrural joints and the talocalcaneal (subtalar) joints, allows movements along several axes of motion.1 Dorsiflexion and plantar flexion of the ankle joint complex occur primarily at the talocrural joints, rotating about the horizontal axis that passes through the medial and lateral malleoli (Fig. 58-3; see also Fig. 58-5). Motions of the ankle joint complex in conjunction with the midtarsal joints include inversion and eversion, which are rotational movements about the oblique subtalar axis involving the subtalar joint (see Fig. 58-3A), and abduction (external rotation) and adduction (internal rotation), which are rotational movements about the longitudinal axis of the tibia (see Fig. 58-3B). The components providing stability to the ankle are best conceptualized as a ringlike structure surrounding the talus2 (Fig. 58-4). Disruption of one element of this ring does not, by itself, induce instability. Injury to one ring element, however, should prompt careful scrutiny for a second injury. Any disruption of two or more elements causes ankle instability and can significantly affect joint function.2 The presence of immediate swelling and severe pain in the ankle region suggests serious ligament disruption, hemarthrosis, or fracture, and rapid progression of symptoms may represent more severe injury. Inability to bear weight immediately after an injury often implies a significant pathologic condition.3 Patient recollection of a “pop” sound should prompt consideration of ligament, tendon, or retinacular rupture but does not necessarily increase the probability of a fracture. Finally, the inciting event causing the ankle injury should be determined and, when necessary, further investigated. The examination of the ankle starts with an assessment of deformity, ecchymosis, edema, and perfusion, followed by active and passive range of motion. Assessment of point tenderness may localize ligament, bone, or tendon injuries, particularly when the patient is seen early. Palpation should include the medial and lateral collateral ligaments, the syndesmotic ligaments, the inferior and posterior edges of the medial and lateral malleoli, the entire length of the fibula and tibia, the anterior plafond, the medial and lateral dome of the talus (palpable with the ankle in plantar flexion), the base of the fifth metatarsal, the calcaneus, the Achilles tendon, and the peroneal tendons behind the lateral malleolus. Stress testing of the ankle joint, which is discussed later, should not be performed until a fracture has been excluded. An evaluation of weight-bearing ability should proceed only if clinical suspicion of a fracture is low, the location of tenderness does not indicate the need for plain radiography, or radiographs have ruled out a fracture.3 Specific clinical examination tests are discussed elsewhere in the appropriate sections. The anteroposterior, lateral, and mortise views make up the standard three-view radiographic series of the ankle. Although two-view ankle series have been studied, the likelihood of missing a subtle fracture is reduced with three views.4 Subtle fractures can be easily missed on ankle radiographs,5 and a standardized approach to radiograph interpretation can reduce the likelihood of missing low-energy ankle fractures6 (Fig. 58-5). The anteroposterior view identifies fractures of the medial and lateral malleoli, anterior tibial tubercle, distal tibia or fibula, talar dome, body and lateral and posterior process of the talus, and calcaneus. The lateral view identifies fractures of the anterior and posterior tibial margins, talar neck, posterior talar process, calcaneus, and any anterior or posterior displacement of the talus or pathology involving the talonavicular joint. On this view, any incongruity of the articular space between the talar dome and the distal tibia suggests ankle instability, particularly if narrowing of the anterior joint space is present. The lateral view is also useful in identifying an ankle effusion, which appears as a teardrop-shaped density displacing the normal fat adjacent to the anterior or posterior margin of the joint capsule. The presence of an effusion suggests the possibility of a subtle intra-articular injury, such as an osteochondral lesion of the talar dome.7 The mortise view, which is taken with the ankle in 15 to 25 degrees of internal rotation, is most important for evaluating the congruity of the articular surface between the dome of the talus and the mortise. The lines formed between the articular surfaces should be parallel, the joint space should appear uniform throughout the tibiotalar and talofibular components of the joint, and the medial clear space should not exceed 4 mm8 (Fig. 58-6). In most cases of isolated blunt ankle trauma evaluated within 48 hours of injury, the Ottawa Ankle Rules (OAR) should be used to determine whether ankle or foot radiographs are necessary.3,9 The OAR state that an ankle radiographic series is required if there is pain in the malleolar region with any of the following findings: • Bone tenderness at the posterior edge of the distal 6 cm or the tip of the lateral malleolus, or • Bone tenderness at the posterior edge of the distal 6 cm or the tip of the medial malleolus, or • Inability to bear weight (defined as the ability to transfer weight onto each leg regardless of limping) for at least four steps both immediately after the injury and at the time of evaluation • Bone tenderness at the navicular bone, or • Bone tenderness at the base of the fifth metatarsal, or • Inability to bear weight for at least four steps both immediately after the injury and at the time of evaluation The OAR have a sensitivity approaching 100% in detecting malleolar zone ankle fractures and midfoot zone fractures.3,9 The OAR were derived in an adult population and are not applicable in subacute or chronic injuries. The OAR appear to perform well in pediatric patients older than 5 years; however, results have varied, leading some researchers to propose alternative rules to address the unique aspects of this population.10–18 The decision rules for foot radiography, although applicable to blunt ankle trauma, apply only to the midfoot zone. The OAR were not designed to be general guidelines for foot radiography and certainly do not apply to the hindfoot or forefoot. Finally, the OAR are not applicable to intoxicated patients or those who are difficult to assess because of head injuries, multiple injuries, or diminished sensation related to neurologic deficits. Use of the OAR by specialized emergency and triage nurses has been found to have efficacy in application comparable to that for use by physicians.19–21 Although the OAR are well validated, their adoption and clinical impact remains variable.22,23 Although plain radiography is the initial imaging modality of choice for ankle injuries, it can miss subtle ankle fractures, osteochondral lesions, stress fractures, or ligamentous injuries. When unexplained symptoms persist after negative or inconclusive findings on plain radiography, other imaging modalities or orthopedic consultation may be advisable.24 Radionuclide imaging (bone scanning) can detect soft tissue injuries, such as distal syndesmotic disruptions, stress fractures, and osteochondral lesions.25 Bone scan abnormalities are present once a patient is symptomatic and typically appear 1 to 2 weeks before radiographic evidence of a stress fracture. Because of its high sensitivity, a negative bone scan effectively rules out the diagnosis. Bone scan abnormalities are nonspecific, however, because infections and tumors also can lead to positive results (see further discussion on stress fracture imaging in the “Foot” section of this chapter), and bone scanning is not useful for follow-up because abnormalities can persist for up to 1 year after recovery.25 Radionuclide imaging is virtually always ordered on an outpatient basis and has been largely supplanted by computed tomography (CT) and magnetic resonance imaging (MRI). CT scanning provides superior bone imaging and is an excellent modality to delineate abnormalities not identified or incompletely characterized by other imaging techniques.24,25 CT can detect small fractures, subtle stress fractures, and ligamentous injuries and can facilitate surgical planning.24,25 Newer CT image reformatting techniques can be extremely helpful, including two-dimensional multiplanar reformatting to identify small fractures, three-dimensional volume rendering to show relationships between tendons and underlying bones, and shaded surface display to provide disarticulated views of joint surfaces and enhance diagnostic accuracy.26,27 MRI, although not typically performed emergently, provides unprecedented clarity in depicting soft tissue structures such as ligaments and tendons and can also delineate bone marrow changes associated with stress fractures before radiographic abnormalities appear.25 MRI can be helpful both in guiding management decisions and in following the patient’s response to therapy.28 Additional imaging techniques such as magnetic resonance or CT arthrography can be useful in the evaluation of chronic ankle pain to detect loose bodies, ligamentous injuries, cartilaginous abnormalities, impingements, or osteochondral lesions.29 CT/SPECT, which combines CT and radionuclide scanning with single photon emission computed tomography (SPECT), has been shown to significantly increase the diagnostic ability of imaging in osteochondral lesions, stress fractures, impingement syndromes, and osteomyelitis.30 The decision to perform specialized imaging of this nature is typically made through orthopedic or radiologic consultation; such studies are not performed in the emergency department (ED). Pathophysiology: Fractures occur when a deforming force is sufficient to overcome the structural strength of a bone. A bone under tension breaks transversely along the axis of the deforming force31 (Fig. 58-7). Alternatively, ligamentous rupture or an avulsion fracture can occur at either end of a stressed ligament or tendon. Management: The management of ankle fractures consists of identification and classification, assessment of stability, immediate reduction of fracture-dislocations that threaten soft tissues or neurovascular status, and specific treatment and disposition. To date, no ideal system has been developed for the classification of ankle fractures. The classic Danis-Weber (Fig. 58-8) and Lauge-Hansen classification systems are based on fracture location and mechanism of injury, respectively.32 The Danis-Weber classification has predictive value for operative repair in isolated lateral malleolar fractures, as the location of the fibular fracture is related to the integrity of the syndesmosis, and is thus more useful to emergency physicians than the more complex Lauge-Hansen classification. Both systems have limitations, however, and neither accurately predicts management or clinical outcome in all situations. The Danis-Weber system does not adequately classify isolated medial malleolar fractures, bimalleolar, trimalleolar, or pilon fractures.33 By contrast, the Lauge-Hansen classification was intended to characterize ligamentous injury patterns based on the radiographic appearance of ankle fractures.34 According to a recent MRI study of 49 ankle fractures, however, this system was unable to predict patterns of ligamentous injuries in 53% of cases, and 17% of cases were unclassifiable.35 This study also found that more than 65% of cases had a complete ligamentous disruption associated with a related malleolar fracture, calling into question the stability of the fractures. It is clear that the Lauge-Hansen system in isolation is inadequate for classifying all fractures and has particular limitations in predicting soft tissue injuries. Modifications to these two classification schemes have been proposed to better describe ankle fractures and, more important, to predict outcome; however, because of their complex nature, most modified classification schemes are relegated to research applications and trauma registries.33–35 The injured ankle should be promptly immobilized, elevated, and iced to minimize swelling and further soft tissue damage. The presence of gross deformity with neurovascular compromise or skin tenting necessitates immediate intervention.36,37 Plain radiography before reduction can be helpful but should not delay reduction in injuries with obvious vascular compromise. Disposition: In general, all displaced or potentially unstable ankle fractures require orthopedic consultation in the ED (Box 58-1). These injuries include all bimalleolar and trimalleolar fractures and unimalleolar fractures with contralateral ligamentous injuries (e.g., a lateral malleolar fracture with deltoid ligament disruption or a medial malleolar fracture with lateral collateral ligament disruption).38 In addition, all intra-articular fractures, especially those with step deformity of the articular surface, require early orthopedic involvement. Extra-articular fractures that disrupt only one ring element generally can be treated with casting for 6 to 8 weeks. Orthopedic follow-up on an outpatient basis within 1 to 2 weeks of the injury is ideal in case operative intervention is required. The presence of any abnormal measurement on the mortise view (see Fig. 58-6) suggests instability and the need for orthopedic consultation in the ED. Avulsion fractures, in which the avulsed fragment is less than 3 mm in diameter and minimally displaced, can be treated in an identical manner to an ankle sprain. The outcome of ankle fractures depends on the extent of injuries, the number of malleoli fractured, ankle stability, and patient age.32,33 For ankle fractures that require surgery, outcome is better in unimalleolar fractures over trimalleolar fractures, in isolated lateral malleolar fracture over isolated medial malleolar fractures, in multimalleolar fractures without medial malleolar fracture over those with malleolar fractures, and in cases with posterior fragments involving less than one third of the articular surface over larger fragments.39 Lateral Malleolar Fractures.: The stability of an isolated lateral malleolar fracture depends on the location of the fracture in relation to the level of the tibiotalar joint, which defines the distal portion of the syndesmotic ligament and the stability it provides to the ankle joint. The Danis-Weber classification (see Fig. 58-8) is useful and predictive of outcome in these types of unimalleolar fractures.33 This classification groups fractures into three groups (A, B, and C), each of which has three subgroups. Lateral malleolar fractures below the tibiotalar joint (Danis-Weber type A) rarely disrupt other bony or ligamentous structures, and in the absence of injury to the medial structures such fractures are unlikely to affect the dynamic congruity of the ankle joint.38 The management of uncomplicated lateral malleolar fractures involves casting for 6 to 8 weeks, with no weightbearing for at least the first 3 weeks, and ongoing follow-up to ensure proper union. Concomitant tenderness over the deltoid ligament may suggest a biomechanical disruption of both malleoli, an associated fracture of the medial malleolus, or an associated fracture of the posterior malleolus and warrants orthopedic consultation in the ED, especially if the medial clear space on the mortise view is widened (see Fig. 58-6).38 CT imaging can be useful in such situations as it may identify occult medial or posterior malleolar fractures. Fibular fractures proximal to the tibiotalar joint line (a Danis-Weber type C injury; see Fig. 58-8) frequently, but not always, disrupt the distal tibiotalar syndesmosis and the medial structures and commonly require orthopedic consultation in the ED and operative intervention. Treatment of an isolated fracture at the level of the tibiotalar joint (a Danis-Weber type B injury; see Fig. 58-8) is controversial because 50% of these injuries are accompanied by an injury to the distal tibiofibular syndesmosis that may require operative intervention.40 Distal tibiofibular space measurements on plain radiography have a sensitivity of only 31% and a specificity of 83%, compared with CT scan, in detecting tibiofibular syndesmosis injuries.41 Tenderness on palpation of the syndesmotic ligament or a widening of the medial joint space on the mortise view adds further support to the need for emergency consultation. Medial Malleolar Fractures.: Medial malleolar fractures are usually the result of eversion or external rotation. These two forces exert tension on the deltoid ligament, causing an avulsion of the tip of the medial malleolus or a rupture of the deltoid ligament. Although they can occur in isolation, medial malleolar fractures are commonly associated with lateral or posterior malleolar disruption. Because of this, the identification of a medial malleolar fracture warrants a careful examination of the entire length of the fibula for tenderness, the presence of which warrants radiographic evaluation to rule out a proximal fibular fracture (Fig. 58-9). An isolated nondisplaced medial malleolar fracture can be treated with casting for 6 to 8 weeks, with no weightbearing for at least the first 3 weeks and close orthopedic follow-up. Any displacement or concomitant disruption of the lateral components of the ankle warrants orthopedic consultation in the ED for consideration of operative management.38 Posterior Malleolar Fractures.: Isolated fractures of the posterior malleolus are rare and imply an avulsion of the posterior tibiofibular ligament. These injuries can be associated with proximal fibular fractures and medial and lateral collateral ligament sprains. Treatment usually consists of casting for 6 weeks, provided that no associated injury or ankle instability is present.42 Fractures involving more than 25% of the tibial surface usually require open reduction and internal fixation.38 Bimalleolar Fractures: Bimalleolar fractures involve the disruption of at least two elements of the ankle ring and are therefore unstable. These fractures result from adduction or abduction forces, the latter being more common.31 Rotational injuries also can cause bimalleolar fractures, as well as trimalleolar fractures if the posterior malleolus is involved. The mechanism of injury often can be deduced from the appearance of the fractures.31 An abduction injury exerts tension on the medial malleolus, causing a horizontal fracture, and compresses the lateral malleolus, causing an oblique shear or a comminuted fracture (see Fig. 58-7). An adduction injury causes the reverse, leading to a horizontal fracture of the fibula and an oblique shear fracture of the medial malleolus. A rotational injury causes oblique or spiral fractures of the fibula or medial malleolus. Associated damage to other soft tissue structures (e.g., the syndesmosis) is common with bimalleolar fractures. Controversy exists about whether such injuries should be treated closed or surgically.31,43 Unstable bimalleolar fractures require surgical intervention, however, and one study found that outcomes at 1 year after surgery were worse with bimalleolar fractures than with lateral malleolar fractures with deltoid ligament disruption.44 Rarely, stress fractures of the medial malleolus or distal fibula can be seen, particularly in athletes and runners. Plain radiographs may be nondiagnostic, but radionuclide bone scanning, CT, or MRI—the choice of which is often influenced by local availability—can establish the diagnosis.45 Most such injuries can be treated nonoperatively, but orthopedic consultation and follow-up are prudent. Open ankle fractures usually occur from severe isolated ankle injuries or multiple trauma and require immediate orthopedic consultation. After documentation of the neurovascular status and the extent of soft tissue trauma, gross contaminants should be removed from the wound, saline-soaked sterile gauze should be applied, and the injured leg should be splinted.36 Swabbing an open wound for bacterial culture and sensitivity testing is unnecessary. If significant deformity is present, immediate reduction before splinting is indicated.36 Tetanus immunoprophylaxis should be administered as appropriate. Because open fractures are invariably contaminated with bacteria, patients with these injuries should receive intravenous antibiotics.47,48 For low-energy injuries with mild to moderate contamination, a first-generation cephalosporin is usually sufficient.36,47,48 Heavily contaminated wounds require the addition of gram-negative bacterial coverage, typically an aminoglycoside.47,48 Adding either penicillin G or clindamycin (if penicillin allergic) as a third antibiotic is necessary for farm- or soil-related crush injuries, in which contamination with Clostridium perfringens can be present.47,48 In addition to the ankle radiographs, radiographs of the foot, tibia, and fibula should be obtained. All open fractures benefit from early surgical intervention for débridement and irrigation.36 Therefore identification is crucial, and emergency orthopedic consultation must be sought for such injuries. Complications: Early operative complications of closed and open ankle fractures include pin site infection, delayed skin necrosis, skin graft rejection, and osteomyelitis. Delayed complications of both operative and nonoperative treatment include malunion, nonunion, osteopenia, traumatic arthritis, chronic instability, ossification of the interosseous membrane, avascular necrosis, and complex regional pain syndrome.2,49 Pilon fractures involve the distal tibial metaphysis and usually are the result of high-energy mechanisms, such as falls from a significant height. These injuries often are comminuted and associated with significant soft tissue trauma, devastation of joint architecture, and leg shortening (Fig. 58-10). Other, higher-priority injuries can be present in such situations. Pathophysiology: Destot first coined the term hammer fracture to describe the way the head of the talus drives itself into the tibial plafond and causes a pilon fracture. The primary deforming force is one of axial compression, and the position of the foot at the time of injury determines the fracture location and pattern50 (Fig. 58-11). Secondary rotational or shear forces may cause increased comminution and fragment displacement with more extensive soft tissue injuries. One fourth of pilon fractures are open, and associated injuries include fractures of the calcaneus, tibial plateau, femoral neck, acetabulum, or lumbar vertebrae, as well as trauma to other major systems. Management: Radiographic examination should include the entire tibia and fibula, as well as the ankle. The emergency management principles for open fractures, as outlined previously, should be applied. Treatment involves restoration of the articular surface and fibular length, combined with meticulous management of soft tissue injuries.50,51 Because surgical management is required, orthopedic consultation in the ED is necessary. Pilon fractures with low-grade soft tissue damage are managed with primary open reduction and internal fixation.51,52 In severe pilon fractures with extensive soft tissue damage, however, results are better with a two-stage approach involving initial length restoration and external fixation followed by anatomic reduction and internal fixation after soft tissue swelling has subsided.52–54 Complications: Complications of pilon fractures are common, particularly in more severe cases.51 Early complications include wound infection, skin sloughing, pin site infection, and wound dehiscence. Delayed and late complications include malunion, nonunion, leg shortening, post-traumatic arthritis, avascular necrosis, and protracted pain. Some patients with severe pilon fractures ultimately require arthrodesis. Ligament Injuries: Ankle sprains are commonly seen in EDs, with a recent series estimating an annual incidence of 52.7 to 60.9 cases per 10,000 population.55 Ankle sprains also are one of the most common injuries in young athletes, and 40% of patients experience dysfunction for up to 6 months postinjury.56,57 The term ankle sprain refers to a potpourri of ligamentous and nonligamentous injuries.58 Even when ligamentous injury is certain, the ideal treatment approach remains controversial, and significant variation in clinical practice exists.55,59,60 Pathophysiology.: Most ankle sprains occur from extreme inversion and plantar flexion causing symptoms on the lateral aspect of the ankle. Usually the anterior talofibular ligament is injured first, followed by the calcaneofibular ligament if the deforming forces are sufficiently strong (see Fig. 58-1). Approximately two thirds of ankle sprains are isolated anterior talofibular ligament injuries, whereas 20% involve both anterior talofibular and calcaneofibular ligament injuries. In addition, the lateral talocalcaneal ligament may be stressed with an inversion injury, leading to avulsion fractures at either end of the attachment sites.61 Isolated calcaneofibular or posterior talofibular ligament injuries are rare. Injuries of the distal tibiofibular syndesmotic ligaments are uncommon in the general population but may represent 10 to 20% of injuries in competitive athletes.62 Dorsiflexion and external rotation forces are usually responsible for this injury, the presence of which may significantly prolong the recovery time from lateral collateral ligament sprains.62 Ligamentous injuries are classified into three grades based on functional and presumed pathologic findings. A grade I injury involves ligamentous stretching without grossly evident tearing or joint instability. A grade II injury involves a partial tear of the ligament with moderate joint instability, often accompanied by significant localized swelling and pain. A grade III injury involves a complete tear of the ligament with marked joint instability, severe edema, and ecchymosis. This classification system, although commonly used, fails to characterize ankle injuries involving two or more ligaments, and it does not consider nonligamentous injuries. Although more comprehensive classification systems have been proposed,61 there is a strong association with increased gradation of ankle sprain and long-term risk of chronic instability, early osteoarthritis, chronic pain, and permanent disability.63,64 Clinical Features.: Although desirable, an accurate history of ankle position and injury mechanism is often unavailable. Inversion followed by external rotation of the ankle suggests the potential for deltoid or syndesmotic injury. Forced dorsiflexion with snapping may indicate peroneal tendon displacement. Previous injuries to the same ankle or symptoms of recurrent ankle instability or pain suggest the presence of a subacute or chronic pathologic process. On physical examination, the presence of edema, ecchymosis, and point tenderness over the medial or lateral collateral ligaments or the syndesmotic ligaments suggests a ligamentous injury. Inability to bear weight in the absence of a fracture suggests the presence of a grade II or III ankle sprain.65 With inversion injuries, point tenderness may also be present along the distal fibula, the lateral aspect of the talus, the lateral aspect or anterior process of the calcaneus, or the base of the fifth metatarsal. Deltoid ligament tenderness necessitates palpation of the full length of the fibula to rule out a proximal fibular fracture (a type C Danis-Weber or Maisonneuve fracture; see Figs. 58-8 and 58-9) and a low threshold for imaging the entire tibia and fibula should exist. The fibular compression test, also known as the squeeze test, reveals fibular and syndesmotic injuries.62 To perform this test, the examiner places the fingers over the fibula and the thumb over the tibia at midcalf and squeezes the two bones. Pain anywhere along the length of the fibula suggests a fibular fracture or an interosseous membrane or syndesmotic ligament disruption at that location.62 Finally, the Achilles tendon should be assessed. Diagnostic Strategies: Radiology.: Standard ankle radiographic views are useful to exclude fractures and to detect instability by the measurement of joint spaces (see earlier discussion and Fig. 58-6).8 Presence of avulsion fractures, which can be located at the bases of the malleoli, the lateral process of the talus, the lateral aspect of the calcaneus, the posterior malleolus, the lateral aspect of the distal tibia, or the base of the fifth metatarsal, constitute an important clue to the location of ligamentous injuries. In addition to the standard mortise measurements previously discussed, two measurements on the anteroposterior radiograph further evaluate the distal tibiofibular syndesmosis (see Fig. 58-6).8 At the distal overlap between the fibula and the tibia, the distance between the posterior edge of the lateral tibial groove and the medial fibular cortex (syndesmosis A) should not exceed 5 mm.8 Furthermore, the amount of tibiofibular bony overlap (syndesmosis B) should be at least 10 mm.8 Measurements outside of these values suggest a syndesmotic diastasis. Stress radiographs, accomplished by taking radiographs during stress testing of the ankle, generally do not influence the emergency management of ankle sprains and are not recommended.66 Many injuries can masquerade as ankle sprains.58 Box 58-2 lists conditions to be considered in the differential diagnosis; Figure 58-12 shows locations of common fractures in or near the ankle that can be misdiagnosed as an ankle sprain. Management.: Most ligament sprains, regardless of severity, heal well and result in a satisfactory outcome. To date, compelling evidence for a significant difference in outcomes between surgical and functional (nonsurgical) treatment is lacking. Limited data suggest that recovery times may be longer and complications more frequent with surgical treatment.67 Most patients with acute sprains of the ankle should start with functional treatment.68 For the minority who fail to respond, delayed operative repair of ruptured ligaments, sometimes years after the injury, has been shown to yield results equivalent to those with primary repair.68,69 Functional treatment, which is defined as a form of therapy in which the ankle is not fully immobilized, allowing either complete or partial joint function, starts in the ED with RICE therapy (rest, ice, compression, and elevation); however, significant variability exists in how this combination is applied, and the optimal methods remain unclear.60,61,70 The evidence to date suggests that lace-up ankle support is more effective in short-term edema reduction than semirigid ankle support, elastic bandaging, and taping. Elastic bandaging causes fewer complications than taping but appears to correlate with slower return to work and sports.60 One study suggests that compared with elastic bandaging, ankle bracing with a lace-up brace such as the Air-Stirrup Ankle Brace (Aircast, DJO Inc., Vista, Calif.) leads to improved functioning at both 10 days and 1 month.71 For grade I or II injuries, short-term protection with a tensor bandage, taping, a laced-up support, or a commercial walking boot or brace, with the optional use of crutches for a few days, is appropriate.68,70 For patients with first-time ankle sprains, treatment with a lace-up stirrup brace combined with elastic wrapping results in an earlier return to function compared with use of a brace alone, elastic wrap alone, or a walking cast.72 For severe grade II or grade III injuries, there is currently equipoise regarding the merit of immobilization compared with functional rehabilitation, with little high-quality evidence to guide therapy.73,74 A recent study supports a 10-day period of immobilization with a below-knee cast or Aircast ankle brace to speed recovery from ankle sprains, with immobilization leading to reduced symptoms and faster recovery compared with tubular compression bandages.75 However, a weakness in this study was the lack of a control group incorporating an active ankle physiotherapy program, known to be important for improved recovery. An accelerated functional rehabilitation program carried out over the first week of injury has also recently been shown to improve function in grade I and II ankle sprains in the short term.76 Because there is little evidence for a more favorable outcome with complete immobilization over functional treatment incorporating a removable brace, the use of a lace-up support or air cast that permits some ankle motion is generally preferable.68,74,77 Such patients should also use crutches to avoid weightbearing until they can stand and walk a few steps on the injured ankle without pain. How long crutches will be required varies significantly, ranging from a few days to 2 or 3 weeks. Follow-up care with the patient’s primary physician within the first 2 weeks is appropriate for minor sprains, whereas orthopedic or sports medicine referral on an outpatient basis is prudent for severe sprains. Analgesics are often necessary for pain management in ankle injuries, and studies suggest that nonsteroidal anti-inflammatory agents, acetaminophen, or oral opioids for severe cases are efficacious.78–80 Topical diclofenac gel also has been shown to have efficacy in pain reduction and allowing early mobilization.67,81,82 After the acute management phase, the next two phases of functional treatment involve appropriate early rehabilitation and occur outside the ED.83 Phase two, which begins after swelling has subsided and the patient is able to bear weight easily, involves strengthening the peroneal and dorsiflexor muscles by isometric, concentric, and eccentric exercises. The final phase begins when full range of motion has been reestablished and the patient can exercise painlessly. This starts with exercises to rebuild motor coordination and proprioception, recondition the muscles, and increase endurance. The patient uses an ankle tilt board or disk to develop coordination and performs increasingly demanding functional activities (e.g., brisk walking, running, and figure-of-eight running to hopping, jumping, and cutting) to build up the muscle groups.83,84 With severe sprains the patient may benefit from the use of air casts, braces, or taping during the latter two phases of functional treatment and in the initial period of return to sports.83 The entire treatment program usually lasts 4 to 6 weeks, depending on the injury’s severity.61,70,85 Disposition.: Rarely, orthopedic consultation in the ED is indicated for an acute ligament sprain. Primary surgical repair of acute ligament rupture is controversial, and possible indications include sprains with displaced osteochondral lesions, complete tears of both the anterior talofibular and calcaneofibular ligaments in a young athlete, a ligament sprain associated with a fracture causing instability (e.g., a deltoid ligament rupture with a lateral malleolar fracture), and an acute severe sprain in a patient with a history of recurrent and severe sprains.61 Failure of nonoperative treatment also constitutes an indication for surgical repair; however, an orthopedic referral on an outpatient basis is adequate ED management.69 Despite appropriate treatment, chronic problems develop in 10 to 30% of patients with ankle sprains.70 These include functional instability, mechanical instability, chronic pain, stiffness, and recurrent swelling and occur more often in grade III ankle sprains. Functional instability refers to the patient’s subjective sensation that the ankle gives way during activity. Although this may be a minor nuisance for some people, it can be devastating and debilitating for persons whose activities demand a high degree of ankle stability. Mechanical instability results from ligamentous laxity, which allows ankle joint movements beyond the physiologic range. In contrast to functional instability, mechanical instability can often be demonstrated clinically by the anterior drawer or talar tilt test and stress radiographs.61 Soft tissue abnormalities that cause chronic pain include synovial impingement, peroneal tendon subluxation or dislocation, intra-articular loose bodies, anterior tibiofibular syndesmotic ligament injuries, and degenerative arthritis. Bone-related causes of chronic pain include osteochondral lesions, fractures of the anterior process of the calcaneus, fractures of the lateral process of the talus, and anterior and posterior impingement.58,86 Achilles Tendon Rupture.: Achilles tendon rupture is most common in middle-aged men, and its causes are multifactorial. This condition is easily misdiagnosed, leading to a delay in therapy, a worse prognosis, and increased morbidity, including chronic weakness and loss of function. In the great majority of cases, a complete transection of the tendon is present; however, partial tears of the Achilles tendon can occur and may be more prone to misdiagnosis. Achilles tendon rupture results from direct trauma or indirectly transmitted forces, including sudden unexpected dorsiflexion, forced dorsiflexion of a plantar-flexed foot, and strong push-off of the foot with simultaneous knee extension and calf contraction (as in a runner accelerating from the starting position). Factors predisposing to Achilles tendon rupture include preexisting disease such as rheumatoid arthritis, systemic lupus erythematosus, gout, hyperparathyroidism, or chronic renal failure, steroid use or injection, fluoroquinolone antibiotic therapy, and previous Achilles tendon rupture.87 The diagnosis of Achilles tendon rupture is primarily clinical. Patients usually describe a sudden onset of pain at the back of the ankle associated with an audible “pop” or “snap.” Although the pain can resolve rapidly, weakness in plantar flexion persists. On examination, a visible and palpable tendon defect may be noted 2 to 6 cm proximal to the calcaneal insertion in acute presentations but will be less apparent in delayed presentations because of hematoma or edema. Even in cases of complete Achilles tendon rupture, weak plantar flexion may still be possible because of the actions of the tibialis posterior, toe flexors, and peroneal muscles. This retained ability for plantar flexion often leads to the misdiagnosis of complete ruptures as ankle strains or partial tears in as many as 25% of cases.88 The classic maneuver to assess the integrity of the Achilles tendon is the Thompson test.89 This is performed with the patient prone and the knee flexed at 90 degrees or the feet hanging over the end of the stretcher. Alternatively, the patient kneels on a chair with both knees flexed at 90 degrees and the feet hanging over the edge. Squeezing the calf muscles in these two positions should cause passive plantar flexion of the foot. Absence of this motion, or a markedly weakened response compared with the uninjured side, suggests complete rupture. Another recently described diagnostic test, the reverse Silfverskiöld test, compares dorsiflexion of the injured ankle with that in the uninjured ankle while the patient is in the supine position. Achilles tendon rupture results in a notably increased degree of dorsiflexion compared with the uninjured side.90 Lateral radiographic views of the ankle may suggest rupture by showing opacification of the fatty tissue–filled space anterior to the Achilles tendon (Kager’s triangle) or an irregular contour and thickening of the tendon.88 Ultrasonography or MRI can demonstrate partial or complete tendon ruptures, but these studies are indicated only in cases in which diagnostic uncertainty exists.88 A lack of consensus exists regarding the choice between operative and nonoperative management in the treatment of Achilles tendon rupture.91–93 Surgical repair is routinely performed in active individuals owing to its lower incidence of rerupture. However, surgery carries higher rates of other complications, such as superficial or deep wound infections, in comparison with nonoperative management.91,94 In both types of management, early mobilization improves functional recovery without increasing rerupture rates.91,93 Minimally invasive surgery combined with early rehabilitation with postoperative functional bracing may further improve outcome.95,96 Achilles tendon rerupture after initial nonoperative treatment usually necessitates surgical repair, with substandard results compared with primary repair.97 ED orthopedic referral of patients with Achilles tendon rupture is necessary to determine the appropriate management. Peroneal Tendon Dislocation or Tear.: The peroneal muscles are the primary evertors and pronators of the foot and also participate in plantar flexion. The peroneus longus and brevis tendons use the posterior peroneal sulcus (the fibular groove), located behind and underneath the lateral malleolus, as a pulley for their midfoot insertions. The peroneus brevis tendon inserts onto the tuberosity of the fifth metatarsal, and the peroneus longus tendon courses beneath the cuboid to insert onto the medial cuneiform and base of the first metatarsal. The superior peroneal retinaculum (Fig. 58-13), a fibrous structure running from the distal fibula to the posterolateral aspect of the calcaneus, maintains the peroneal tendons against the fibular groove. Anterior subluxation or dislocation of the peroneal tendons occurs as a result of a tear of the superior peroneal retinaculum attachment from the fibula.98,99 This infrequent injury is commonly misdiagnosed as an ankle sprain and can occur in isolation or concomitant with other sprains or fractures. The mechanism of injury usually is forced dorsiflexion with reflex contraction of the peroneal muscles, resulting in avulsion of the retinaculum and anterior displacement of the peroneal tendons.98 Patients with a peroneal tendon dislocation complain of sudden pain and a snapping sensation over the posterolateral ankle associated with weakness of eversion. Tenderness and swelling over the lateral retromalleolar area (a location not typically involved in ankle sprains) are characteristic. When accurate examination is not precluded by swelling, the dislocated tendons also may be palpable near the inferior tip of the lateral malleolus. Inability to actively evert the foot when it is held in dorsiflexion or frank subluxation of the tendons with this maneuver confirms the diagnosis. Findings on plain radiography are often normal; however, 15 to 50% of patients will be found to have an associated avulsion fracture of the lateral ridge of the distal fibula. An MRI study or ultrasound can be helpful in confirming the diagnosis. All patients with a suspected or confirmed peroneal tendon dislocation should be referred for orthopedic follow-up because these injuries require surgical repair.99,100 Spontaneous healing is rare in untreated cases, and chronic ankle instability and pain are common sequelae. Peroneal tendons also can tear longitudinally; such injuries manifest either acutely or subacutely with recurrent pain and swelling during activities.100,101 Tibialis Posterior Tendon Rupture.: The tibialis posterior is primarily responsible for plantar flexion and inversion along the subtalar joint. Its tendon uses the posteroinferior surface of the medial malleolus as a pulley and inserts onto the navicular, the medial cuneiforms, and the bases of the second through the fifth metatarsals. The peroneus brevis opposes the action of the tibialis posterior. With rupture of the tibialis posterior tendon, the peroneus brevis becomes unopposed and the medial longitudinal arch loses its muscular support, leading to valgus deformity of the hindfoot and a unilateral flatfoot.102 The mechanism of traumatic tibialis posterior rupture involves forced eversion.102 In addition to a unilateral flatfoot, pain and swelling on the medial aspect of the ankle are seen. Tenderness is present over the navicular, and the patient cannot perform a toe raise on the affected side. In addition, the patient with a tibialis posterior tendon rupture is unable to invert the foot when it is in plantar flexion and eversion. With a unilateral flatfoot, an observer standing behind the patient can see “more toes” on the lateral aspect of the affected side—a classic sign.102 Plain radiography can exclude other bone abnormalities. Ultrasonography and MRI are useful imaging modalities to diagnose this condition.102 Orthopedic consultation is indicated for tibialis posterior tendon ruptures, because surgical repair often is necessary. Other Tendon Injuries.: The tibialis anterior is the primary dorsiflexor of the foot. Its tendon courses under the superior extensor retinaculum and inserts onto the navicular, the medial cuneiform, and the base of the first metatarsal. Tenosynovitis of the tibialis anterior tendon is associated with overuse and characterized by swelling, tenderness, and crepitus along the tendon. Treatment involves RICE therapy, analgesia, and close follow-up. Rupture of the tibialis anterior is rare and often is misdiagnosed as lumbosacral radiculopathy or peroneal nerve palsy because of the footdrop it produces. This condition requires orthopedic consultation in the ED because surgical repair is usually necessary. The flexor hallucis longus is responsible for flexion of the great toe and participates in plantar flexion of the foot. Its tendon courses behind the medial malleolus through a fibro-osseous canal and inserts onto the distal phalanx of the great toe. Flexor hallucis longus tendinitis, also called dancer‘s tendinitis, most often occurs at the fibro-osseous canal.103 On examination, tenderness and edema posterior to the medial malleolus are noted, and passive extension of the first metatarsophalangeal (MTP) joint causes significant pain when the foot is in neutral position. Initial treatment involves rest, nonsteroidal anti-inflammatory drugs, and a short course of immobilization. Orthopedic follow-up on an outpatient basis should be arranged to ensure proper resolution. Rarely, surgical intervention may be necessary.103 Ankle Dislocations: Ankle dislocations are described according to the direction of displacement of the talus and foot in relation to the tibia. Thus dislocation may be upward, posterior, medial, lateral, posteromedial, or anterior. Medial dislocation is the most common. Most dislocations involve associated ankle fractures; rarely, however, dislocations can occur without fracture. The mechanism in all dislocations begins with axial loading of a plantar-flexed foot, which forces the talus either anteriorly or posteriorly from the ankle mortise. The eventual position of the dislocation depends on the position of the foot at the time of injury and the direction of the displacing force. Ankle dislocations can be closed or open and most commonly result from significant falls, motor vehicle collisions (MVCs), or high-speed sports.37 The neurovascular supply to the foot usually is intact but may be compromised in open dislocations.104 ED management involves the assessment of neurovascular status and tendon function, followed by rapid reduction. Radiographs are helpful but should not delay reduction in cases when vascular compromise or skin tenting is present.37 After appropriate procedural sedation and analgesia, the patient is placed supine and the knee is flexed to 90 degrees. Distraction of the foot, followed by a gentle force to reverse the direction of the dislocation, usually accomplishes the reduction.105 Reassessment of the neurovascular status, splint immobilization, ankle elevation, and postreduction radiography should follow. Open dislocations require the same management as previously discussed for open fractures. The prognosis with an ankle dislocation is usually good, although open fractures are associated with an increased incidence of complications.104,105
Ankle and Foot
Ankle
Anatomy
Pathophysiology
Clinical Features
Physical Examination
Diagnostic Strategies
Other Imaging Techniques
Specific Pathologic Conditions
Open Fractures
Pilon Fractures
Soft Tissue Injuries
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ankle and Foot


Only gold members can continue reading. Log In or Register to continue




