Anesthesia for Orthopedic Surgery
Terese T. Horlocker
Denise J. Wedel
Key Points
Related Matter
Scoliosis
Brachial Plexus Injury
Prone Position
Prone Position Facial
Interscalene Block
Ankle Block
Perioperative management of the patient undergoing orthopedic surgery involves knowledge of the specific orthopedic surgical techniques, including duration, extent, predicted blood loss, and associated complications (including nerve injury). Regional anesthetic techniques allow both intraoperative surgical anesthesia and postoperative analgesia, creating a further subspecialty within orthopedic anesthesia. Another vitally important part of orthopedic anesthesia is patient positioning. Experience and knowledge in positioning the patient are required to produce optimal surgical conditions and avoid potential injuries. Likewise, because orthopedic procedures are frequently associated with major blood loss, the orthopedic anesthesiologist must be experienced in techniques that decrease these risks, able to use intraoperative hypotension and blood salvage techniques, and able to manage transfusion-related complications.
Orthopedic surgical patients usually require early mobilization and rehabilitation, both of which can be expedited by appropriate selection of anesthetic techniques and management of postoperative analgesia. A multimodal approach, often utilizing continuous neuraxial or peripheral neural infusions, is associated with enhanced recovery and improved functional outcome. However, patients undergoing major orthopedic surgery are at risk for venous thromboembolism. Knowledge of the current pharmacologic and mechanical methods of thromboprophylaxis is required to prevent the occurrence of these thromboembolic complications, while potential interactions between anticoagulants and anesthetic drugs or regional anesthetic techniques must be thoroughly understood to reduce the risk of perioperative bleeding and neurologic injury for expanding hematomas.
Preoperative Assessment
The anesthesiologist’s preoperative assessment is crucial to the formulation and execution of the anesthetic plan. The patient must be evaluated for pre-existing medical problems, previous anesthetic complications, potential airway difficulties, and considerations relating to intraoperative positioning.
Progression of cardiac symptoms and exercise tolerance in patients with a history of coronary artery disease may be difficult to assess because of the limitations in mobility induced by the underlying orthopedic condition. As a result, pharmacologic functional cardiovascular testing may be warranted. Overall, patients undergoing orthopedic procedures are considered at intermediate risk for cardiac complications perioperatively. Perioperative cardiac morbidity may be decreased by the initiation of β-blockade in selected patients.1
Many patients undergoing orthopedic surgery have rheumatoid arthritis. Systemic manifestations of this disease include pulmonary, cardiac, and musculoskeletal involvement. Particularly significant to the anesthesiologist is involvement of the cervical spine, temporomandibular joint, and larynx. Rheumatoid involvement of the cervical spine may result in limited neck range of motion, which interferes with airway management. Atlantoaxial instability, with subluxation of the odontoid process, can lead to spinal cord injury during neck extension. Patients with rheumatoid arthritis are often receiving chronic steroid therapy and may require perioperative steroid replacement.
The patient’s medications should be reviewed and the patient instructed which medications to continue until the time of surgery. Specifically, antihypertensive medications and chronic opioid therapy should not be discontinued. Patients taking opioids for a period of greater than 4 weeks often develop tolerance and opioid-induced hyperanalgesia, although there can be significant patient variability.2 The patient should also be queried regarding the use of hemostasis-altering drugs; many patients are instructed by their surgeon to begin thromboprophylaxis with aspirin or warfarin preoperatively. Likewise, patients with cardiac-stents may require maintenance of their antiplatelet medications.3
Preoperative evaluation should include a focused physical examination. Patients should be assessed for limitation in mouth opening or neck extension, adequacy of thyromental distance, and state of dentition. The heart and lungs should be auscultated. In addition, the proposed site of needle placement for regional anesthesia should be assessed for evidence of infection and anatomic abnormalities or limitations. A brief neurologic examination, with documentation of any pre-existing deficits, is crucial. At this time, the patient should also be evaluated for any potential positioning difficulties related to arthritic involvement of other joints or body habitus.
Hemoglobin and creatinine values are determined for all patients undergoing major procedures; other laboratory and imaging studies are performed as indicated by preoperative medical conditions. Ideally, the patient should undergo a preoperative educational session in which the surgical procedure, anesthetic/analgesic options, and the postoperative rehabilitative plan are described.
Selection of Anesthetic Technique
Surgery to the Spine
Spinal Cord Injuries
Spinal injury occurs at a rate of 11,000 cases per year (see also Chapter 36). Approximately half of these are at the cervical level. The examination of a person with a suspected spinal cord injury
begins with a prompt neurologic examination and a rapid assessment for possible injury to other systems. Cervical injuries are frequently associated with head injury, thoracic fractures with pulmonary and cardiovascular injury, and lumbar fractures with abdominal and long-bone injuries. The patient should be examined immediately for signs of respiratory insufficiency, airway obstruction, rib fractures, and chest wall or facial trauma.
begins with a prompt neurologic examination and a rapid assessment for possible injury to other systems. Cervical injuries are frequently associated with head injury, thoracic fractures with pulmonary and cardiovascular injury, and lumbar fractures with abdominal and long-bone injuries. The patient should be examined immediately for signs of respiratory insufficiency, airway obstruction, rib fractures, and chest wall or facial trauma.
Serial neurologic examination is necessary to assess the function of the spinal cord above the level of the fracture. The fifth cervical segment is perhaps the most important in providing clinical evidence of cervical spinal injury. This segment controls motor function of the deltoid, biceps, brachialis, and brachioradialis muscles. If these muscles are flaccid, the fifth cervical nerve is involved, and there will be partial diaphragmatic paralysis. A complete lesion at the fourth cervical segment is not compatible with survival unless artificial respiration is initiated. Spinal shock occurs acutely and results in complete cessation of spinal cord functions below the level of the lesion. This results in flaccid paralysis, loss of visceral and somatic sensation, and paralytic ileus. Vasopressor reflexes are also lost. Spinal shock may persist from a few days to 3 months.
Surgical treatment of spinal cord injuries is based on the presence or absence of neurologic function and the radiographic evaluation of vertebral displacement and instability. Patients with unstable spines who are not quadriplegic or paraplegic may become so during transport or positioning for surgery.
Tracheal Intubation
Airway management is critical in patients with cervical spinal cord injury. The most common cause of death with acute cervical spinal cord injury is respiratory failure. All patients with severe trauma or head injuries should be assumed to have an unstable cervical fracture until proven otherwise radiographically. During transport, the patient should be moved on a rigid board with the neck immobilized to prevent further injury. Awake fiberoptic-assisted intubation may be necessary, with general anesthesia induced only after voluntary upper and lower extremity movement is confirmed. Blind nasotracheal intubation may be used if there is no evidence of facial or basal skull fractures. In a truly emergent situation, oral intubation with direct laryngoscopy is the usual approach. The trachea should be intubated with minimum flexion or extension of the neck.
Respiratory Considerations
Ventilatory impairment increases with higher levels of spinal injury. A high cervical lesion that includes the diaphragmatic segments (C4 to C5) results in respiratory failure, and death occurs unless artificial pulmonary ventilation is used. Lesions between C5 and T7 cause significant alterations in respiratory function, owing to the loss of abdominal and intercostal support. The indrawing of flaccid thoracic muscles during inspiration produces paradoxical respirations, resulting in a vital capacity reduction of 60%. Inability to cough and effectively clear secretions results in atelectasis and infection.
Cardiovascular Considerations
During spinal shock, there is loss of sympathetic vascular tone below the injury. If the cardioaccelerator fibers (T1 through T4) are damaged, bradycardia results. Therefore, hemorrhagic shock may not produce a compensatory tachycardia in these patients; the rate may remain at 40 to 60 beats per minute. Monitoring of central venous or pulmonary artery pressures may be necessary for fluid management in a patient with a high cervical lesion. Autonomic instability should be treated with vasoconstrictors, vasodilators, and positive chronotropic drugs as needed.
Succinylcholine-induced Hyperkalemia
Hyperkalemia may develop after administration of succinylcholine to a patient with spinal cord injury. The amount of potassium released depends on the extent of the patient’s motor deficit. It is considered safe to administer succinylcholine for the first 48 hours. After that time, there is a proliferation of acetylcholine receptors in the muscle, and they become supersensitive to depolarizing muscle relaxants.5 The increases in serum potassium are maximal between 4 weeks and 5 months after spinal injury. Serum potassium levels may increase from normal to as high as 14 mEq/L, causing ventricular fibrillation or cardiac arrest. Therefore, succinylcholine should be avoided in all spinal cord–injured patients after 48 hours. There are no contraindications to the nondepolarizing agents.
Temperature Control
Disruption of the sympathetic pathways carrying temperature sensation, and subsequent loss of vasoconstriction below the level of injury, causes spinal cord–injured patients to be poikilothermic. Maintenance of normal temperature can be achieved by applying exogenous heat to the skin, increasing ambient air temperature, warming intravenous fluids, and humidifying gases.
Maintaining Spinal Cord Integrity
All patients with spinal cord trauma should be considered to have compromised spinal cords, and an important component of anesthetic management is the preservation of spinal cord blood flow. Blood pressure and intravascular volume should be maintained within normal levels to ensure adequate spinal cord perfusion pressure. Sustained hypotension may worsen neurologic deficits. Hyperventilation should be avoided because hypocarbia decreases spinal cord blood flow. These considerations, as well as spinal cord monitoring, are discussed in detail later in this chapter.
Autonomic Hyperreflexia
After recovery from spinal shock, 85% of patients exhibit autonomic hyperreflexia when there has been complete cord transection above T5. The syndrome, which can also occur with injuries at lower levels, is characterized by severe paroxysmal hypertension with bradycardia (baroreceptor reflex), dysrhythmias, and cutaneous vasoconstriction below, and vasodilation above, the level of the injury. The episode is typically precipitated by distention of the bladder or rectum, but can be induced by any noxious stimulus. Many patients with spinal injuries and autonomic hyperreflexia will report characteristic headaches with bladder distention. The lack of supraspinal inhibition allows the sympathetic outflow below the lesion to react to the stimulus unopposed. If autonomic hyperreflexia occurs, it should be treated by removal of the stimulus, deepening anesthesia, and administration of direct-acting vasodilators. Untreated, the hypertensive crisis may progress to seizures, intracranial hemorrhage, or myocardial infarction.
Scoliosis
Scoliosis is a deformity of the spine resulting in lateral curvature and rotation of the vertebrae, as well as deformity of the rib cage (Fig. 50-1). The incidence of scoliosis predominantly reflects the incidence of idiopathic scoliosis, which represents 75% to 90%
of cases. The remaining 10% to 25% of cases are associated with neuromuscular diseases and congenital abnormalities, including congenital heart disease, trauma, and mesenchymal disorders. The severity of scoliosis is defined by the angle of scoliosis or Cobb angle. Surgical correction is performed for Cobb angles >50 degrees, with the intent of halting, not reversing, progression of respiratory and cardiac dysfunction. Likewise, quality of life is improved, but only modestly.
of cases. The remaining 10% to 25% of cases are associated with neuromuscular diseases and congenital abnormalities, including congenital heart disease, trauma, and mesenchymal disorders. The severity of scoliosis is defined by the angle of scoliosis or Cobb angle. Surgical correction is performed for Cobb angles >50 degrees, with the intent of halting, not reversing, progression of respiratory and cardiac dysfunction. Likewise, quality of life is improved, but only modestly.
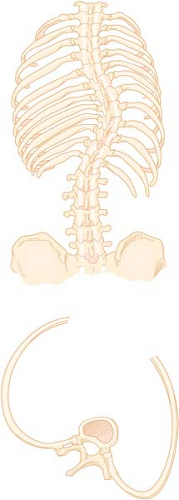 Figure 50.1. Deformity of the vertebrae and rib cage in scoliosis. Primary curvature occurs most frequently in the thoracic and lumbar regions. The vertebral bodies are wedge-shaped, and the posterior angles of the ribs are shallow on the side of concavity. On the convex side, the rib angles are more acute. (Reprinted from: Horlocker TT, Cucchiara RF, Ebersold MJ. Vertebral column and spinal cord surgery. In: Cucchiara RF, Michenfelder JD, eds. Clinical Neuroanesthesia. New York, NY: Churchill Livingstone; 1990:325, with permission.) |
Pulmonary Considerations
The primary abnormality in gas exchange is ventilation–perfusion maldistribution, which contributes to hypoxemia. However, hypercapnia develops with increasing age as compensatory mechanisms fail. Prolonged hypoxia, hypercapnia, and pulmonary vascular constriction may result in irreversible pulmonary vascular changes and pulmonary hypertension. In general, the prognosis of scoliosis associated with neuromuscular disease is worse than that of idiopathic scoliosis. These patients frequently need postoperative ventilatory support.
Cardiovascular Considerations
Cardiovascular function is also affected in patients with scoliosis. At autopsy, these patients exhibit right ventricular hypertrophy and hypertensive pulmonary vascular changes. Prolonged alveolar hypoxia due to hypoventilation and ventilation–perfusion mismatch eventually causes irreversible vasoconstriction and pulmonary hypertension. Scoliosis is also associated with congenital heart conditions, including mitral valve prolapse, coarctation of the aorta, and cyanotic heart disease, suggesting a common embryonic insult or collagen defect.
Surgical Approach and Positioning
The anterior approach to the thoracolumbar spine is achieved with the patient in the lateral position, usually with the convexity of the curve uppermost. Removal of one or more ribs may be necessary for adequate surgical exposure. Likewise, placement of a double-lumen endotracheal tube, with collapse of the lung on the operative side, may be required for surgery above T8. Thus, the thoracolumbar approach for anterior spinal fusion may be associated with more postoperative respiratory insufficiency than posterior fusion because of lung and diaphragmatic manipulation.
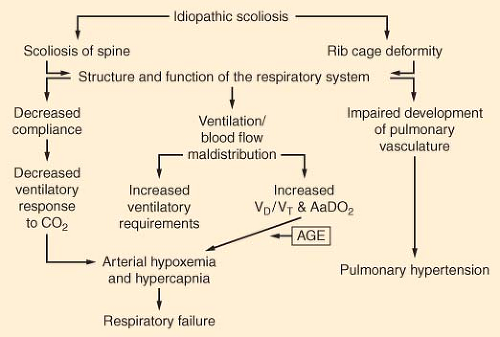 Figure 50.2. The factors in idiopathic scoliosis that contribute to respiratory function abnormalities and failure. VD, dead space volume; VT, tidal volume; AaDO2, alveolar to arterial oxygen gradient. (Reprinted from: Kafer ER. Respiratory and cardiovascular functions in scoliosis. Bull Eur Physiopathol Respir. 1977;13:299, with permission.) |
Combined anterior and posterior spinal procedures yield higher union rates and greater correction in patients undergoing scoliosis correction. It remains unclear whether these two major procedures should be performed on the same day or whether the posterior fusion should be delayed to allow the patient to recover from the anterior (first) procedure. Furthermore, the actual timing of the second procedure remains controversial. Although the degree of correction and the arthrodesis rates are similar for one- or two-stage procedures, the morbidity and number of complications, such as increased blood loss and transfusion requirements, decreased nutritional parameters, and longer hospital stays, may be increased for staged procedures.7 However, these results are not consistent.8 Because the risk of significant complications is present with either same-day or staged anterior–posterior fusion, prospective studies are needed to clarify this issue.
Anesthetic Management
The primary aim of preoperative evaluation of patients with scoliosis is to detect the presence and extent of cardiac or pulmonary compromise. Respiratory reserve is assessed by exercise tolerance, vital capacity, and arterial blood gases. Cardiac studies are performed as indicated to optimize preoperative cardiovascular status. A brief neurologic examination will document pre-existing neurologic deficits. Finally, cervical mobility and upper airway anatomy are assessed to discover any potential airway or positioning difficulties.
 Figure 50.3. Prone position. The head is turned with the dependent ear and eye being protected from pressure. Chest rolls are in place, the arms are brought forward without hyperextension, and the knees are flexed. (Reprinted from: Horlocker TT, Cucchiara RF, Ebersold MJ. Vertebral column and spinal cord surgery. In: Cucchiara RF, Michenfelder JD, eds. Clinical Neuroanesthesia. New York, NY: Churchill Livingstone; 1990:325, with permission.) |
Anesthetic considerations for surgical correction of scoliosis by spinal fusion and instrumentation include management of a patient in the prone position, hypothermia secondary to a long procedure with an extensive exposed area, and replacement of blood and fluid losses, which may be extensive.9 More recently, attention has been focused on the maintenance of spinal cord integrity, prevention and treatment of venous air embolism (VAE), and reduction of blood loss through hypotensive anesthetic techniques.
Adequate hemodynamic monitoring and venous access are essential in the management of patients undergoing spinal fusion and instrumentation. The radial artery is cannulated for direct blood pressure measurement and assessment of blood gases. A central venous catheter is helpful in evaluating blood and fluid management and can be used to aspirate air if VAE occurs. Patients with evidence of pulmonary hypertension, or severe coexistent cardiovascular or pulmonary disease, may require a pulmonary artery catheter.
Degenerative Vertebral Column Disease
Spinal stenosis, spondylosis, and spondylolisthesis are all forms of degenerative vertebral column disease. It is not unusual for more than one of these degenerative changes in the spine to occur concomitantly, leading to a more rapid progression of neurologic symptoms and the need for surgical intervention.
Surgical Approach and Positioning
near critical anatomic structures. Lateral retraction of the carotid artery may endanger blood flow to the brain, particularly in the elderly patient. Retraction of the esophagus and trachea medially may cause pharyngeal laceration, laryngeal edema, and recurrent laryngeal nerve paralysis. Cerebrospinal fluid leaks and trauma to the vertebral artery have also been reported.
In the sitting position for cervical laminectomy, blood flows away from the site of operation, producing a clear operative field and better surgical exposure. In this position, the patient sits with head, arms, and chest supported. The patient must be carefully positioned and the dependent areas must be padded to prevent compression injuries to nerves and skin. Extreme cervical flexion may obstruct the airway. Hypotension can be minimized by gradual attainment of the sitting position. A disadvantage of the sitting position is the increased occurrence of VAE. Although the incidence of VAE in sitting posterior fossa cases is 40%, the incidence is only 5% to 25% in sitting cervical spine procedures.10
Recently, surgical advances have made it possible to perform minimally invasive surgery (MIS) procedures with smaller incisions and decreased soft tissue trauma. MIS techniques can be classified as endoscopic or nonendoscopic (mini-open). Although endoscopic approaches decrease some approach morbidities, they are associated with high instrumentation cost, steep learning curves, and new complication profiles.11,12 Furthermore, the high costs have not been shown to be justified by superior clinical benefits. Nonendoscopic MIS approaches use direct visualization and standard operative techniques and report lower complication rates, reduced length of stay, and faster recovery time. Although certain MIS procedures may produce early cost benefits, longer follow-up, better outcome, and cost data are needed to determine if MIS techniques are cost effective compared to open or nonsurgical interventions.11
Anesthetic Management
Either general or neuraxial anesthesia may be safely administered for relatively uncomplicated lower thoracic and lumbar spine surgery; a randomized trial in 2009 concluded that general anesthesia was associated with higher surgeon satisfaction and less nausea and vomiting.13 General anesthesia is preferred for essentially all thoracic and cervical procedures because of the high spinal level that would be required with a regional technique. General anesthesia ensures airway access, is associated with greater patient acceptance, and can be used for prolonged operations. Succinylcholine should be avoided if there are progressive neurologic deficits.
Spinal Cord Monitoring
The wake-up test, first described by Vauzelle et al.,14 consists of the intraoperative awakening of patients after completion of spinal instrumentation. Surgical anesthesia is typically provided with a balanced technique of nitrous oxide, a volatile drug, and opioids, although use of opioids with a short-acting volatile anesthetic (e.g., sevoflurane), or an infusion of propofol, is also possible. The opioids are important to provide analgesia while the patient is awake and to permit the patient to tolerate the endotracheal tube. During the 30 to 45 minutes before intraoperative wake-up, the volatile anesthetic, or propofol, and muscle relaxants are discontinued and the patient is allowed to awaken gradually. The patient is addressed by name and asked to move both hands, and after a positive response, both feet. Patients usually respond within 5 minutes. If there is satisfactory movement of the hands, but not the feet, the distraction on the rod is released one notch, and the wake-up test repeated. Although recall of the event occurs in only 0% to 20% of patients and is rarely viewed as unpleasant,15 it is important to describe to the patient before surgery what will transpire so that anxiety will be minimized should the patient be fully aware during the wake-up. It is extremely rare for a patient who was neurologically intact when awakened during surgery to have a neurologic deficit on completion of the procedure. However, certain hazards of the wake-up test do exist and include recall, pain, air embolism, dislocation of spinal instrumentation, and accidental tracheal extubation or removal of intravenous and arterial lines.
An adjunct or alternative to the wake-up test is neurophysiologic monitoring. Somatosensory stimulation follows the dorsal column pathways of proprioception and vibration: Pathways supplied by the posterior spinal artery. Accordingly, the motor pathway, which is supplied by the anterior spinal artery, is not addressed by monitoring somatosensory evoked potentials (SSEP). High concentrations of inhaled agents cannot be used when monitoring SSEP. Motor evoked potentials (MEP), in contrast, monitor motor pathways but are technically more difficult to use. Muscle relaxants cannot be used in patients having MEP monitoring. If both SSEP and MEP are to be monitored during spine surgery, one might consider providing anesthesia with an ultrashort-acting opioid infusion with a low-dose inhaled anesthetic and monitoring of the electroencephalogram or bispectral index to minimize the potential for intraoperative awareness. It is of critical importance to note that postoperative paraplegia has occurred despite preservation of intraoperative SSEPs. Combined use of MEPs and SSEPs may increase the early detection of spinal cord ischemia.9,16
Acute alterations in SSEP amplitude or latency signify spinal cord compromise and may be the result of direct trauma, ischemia, compression, or hematoma. If changes occur, it is recommended that surgery be discontinued, blood pressure returned to normal or 20% above normal, and volatile agents decreased or discontinued. Arterial blood gases may be drawn to rule out a metabolic derangement. If the waveform does not return to normal, the surgeon should release distraction on the cord. A wake-up test is often performed at this time to definitely exclude neurologic deficits. In addition to neural injury, SSEPs are altered by volatile anesthetics, hypercarbia, hypoxia, hypotension, and hypothermia.17,18
Blood Loss
exists consistently for positioning and use of tranexamic acid.19,24 However, the safety of antifibrinolytics is not fully known. While tranexamic acid is currently recommended in the adult population, optimal dosing has yet to be determined in pediatric patients.25 Importantly, the FDA has suspended aprotinin use on the basis of safety data in the cardiac literature.19,24
Patients undergoing major spine surgery may acquire a perioperative coagulopathy from dilution of coagulation factors and/or platelets or fibrinolysis. The mechanisms of coagulopathy and the role of coagulation testing during these procedures are poorly defined. However, it appears that a significant deviation from normal values of either the prothrombin time or the activated partial thromboplastin time is predictive of bleeding and may be used to guide transfusion therapy.26 Another rare cause of bleeding during spine surgery is trauma to the aorta, vena cava, or iliac vessels. Unexplained hypotension or signs of hypovolemia without obvious blood loss should alert the anesthesiologist to this possibility.
Visual Loss after Spine Surgery
Ischemic optic neuropathy was the most common cause of visual loss after spine surgery and accounted for 83 of 93 spine surgery cases.30 Using a case control design with multivariate analysis, the American Society of Anesthesiologists Visual Loss Study Group’s risk factors for ischemic optic neuropathy after spinal surgery included male sex, obesity, Wilson frame use, anesthetic duration, increased blood loss, and the use of non-colloid for fluid replacement.31 Using this model, the only preoperative factor that is modifiable is surgical frame selection. In addition, anesthesiologists may use these results to guide fluid administration. It is also recommended that the risk of visual loss should be considered in the preoperative discussion for patients undergoing lengthy spine surgery in the prone position.
Venous Air Embolus
VAE is a catastrophic event that may occur during spine surgery. The large amount of exposed bone and the elevated location of the surgical incision relative to the heart predispose to VAE. Capnography, mass spectrometry, and precordial Doppler are noninvasive, yet effective, in detecting VAE. VAE can occur in all positions associated with laminectomies because the wound is above the cardiac level. Incidences of VAE (defined by aspiration of air through a central venous catheter) in patients undergoing neurosurgical procedures in the sitting, supine, prone, and lateral positions are 25%, 18%, 10%, and 8%, respectively.10 The actual incidence of VAE in spine surgery is unknown; however, poor neurologic recovery is often reported.32 The presenting sign is often unexplained hypotension and an increase in the end-tidal nitrogen concentration, or a precipitous fall in the end-tidal CO2 concentration. The anesthesiologist, therefore, should be aware of the possibilities of VAE because prompt diagnosis and treatment increase patient survival. If VAE is suspected, the wound should be irrigated with saline, nitrous oxide discontinued, and vasopressors administered. Massive embolism may necessitate turning the patient supine and initiating cardiopulmonary resuscitation.
Postoperative Care
Most patients undergoing surgery to the spine can be extubated immediately after the operation if the procedure was relatively uneventful and preoperative vital capacity values were acceptable. Residual opioid or muscle relaxant may lead to hypoventilation or apnea, especially in patients with an associated neuromuscular disease. Some patients who have experienced considerable blood loss and who have received large amounts of intravenous fluids, particularly if they were prone, may have severe facial edema that renders immediate tracheal extubation unwise. Aggressive postoperative pulmonary care, including incentive spirometry, is necessary to avoid atelectasis and pneumonia. Continued hemorrhage in the postoperative period is another concern. Careful monitoring of systemic and central venous pressures, urine output, and wound drainage is essential. Neurologic status must also be monitored closely for deterioration.
Epidural and Spinal Anesthesia after Major Spine Surgery
Previous spine surgery has been considered to represent a relative contraindication to the use of regional anesthesia. The presence of postoperative spinal stenosis or other degenerative changes in the spine or pre-existing neurologic symptoms may preclude the use of regional anesthesia in these patients. Likewise, many of these patients experience chronic back pain and are reluctant to undergo epidural or spinal anesthesia, fearing exacerbation of their pre-existing back complaints. Finally, postoperative anatomic changes make needle or catheter placement more difficult and complicated after major spine surgery; needle insertion can be accomplished only at nonfused segments.
Spread of epidural local anesthetic following spine surgery may be affected by adhesions, producing an incomplete or “patchy” block. Obliteration of the epidural space may increase the incidence of dural puncture and make subsequent epidural blood patch placement impossible. Several retrospective studies have demonstrated that epidural anesthesia may be successfully performed in patients with previous spine surgery; however,
successful catheter placement was possible on the first attempt in only 50% of patients, even with an experienced anesthesiologist. In addition, although adequate epidural anesthesia was eventually produced in 40% to 95% of patients, there appeared to be a higher incidence of traumatic needle placement, inadvertent dural puncture, and unsuccessful epidural needle or catheter placement, especially if spinal fusion extended to L5 through S1.35,36,37
successful catheter placement was possible on the first attempt in only 50% of patients, even with an experienced anesthesiologist. In addition, although adequate epidural anesthesia was eventually produced in 40% to 95% of patients, there appeared to be a higher incidence of traumatic needle placement, inadvertent dural puncture, and unsuccessful epidural needle or catheter placement, especially if spinal fusion extended to L5 through S1.35,36,37
Spinal anesthesia may produce a more reliable block and cause less trauma than epidural anesthesia. Although needle placement may be more difficult or traumatic in these patients, the spread of local anesthetic in the subarachnoid space and quality of block would not be affected. A spinal anesthetic may be more desirable after spine surgery because the technique does not depend on a subjective loss of resistance, but instead has a definite end point— the presence of cerebrospinal fluid.
The overall success and neurologic complication rates was examined in 937 patients with spinal stenosis or lumbar disc disease undergoing neuraxial block, 207 (22%) of whom had previously undergone spine surgery, although the majority were simple laminectomies or discectomies. Success rates did not differ between patients who had previous surgery and those who had undergone a spine procedure. Ten patients experienced new or progressive neurologic deficits when compared with preoperative findings; the neuraxial technique was the primary cause in four patients. The authors concluded that patients with pre-existing spinal canal pathology have a higher incidence of neurologic complications after neuraxial blockade than that previously reported for patients without such underlying pathology.38 These findings validate those of Moen et al.39,40 who reported a higher frequency of (undiagnosed) spinal stenosis in patients who developed paraplegia following uneventful neuraxial block.
Surgery to the Upper Extremities
Orthopedic surgical procedures to the upper extremity are well suited to regional anesthetic techniques. In addition to intraoperative anesthesia, brachial plexus and peripheral nerve blocks may be used in the treatment and prevention of reflex sympathetic dystrophy (complex regional pain syndrome). Continuous catheter techniques provide postoperative analgesia and allow early limb mobilization. Conversely, although the benefits of regional anesthesia in this patient population are well established, orthopedic surgical procedures often involve peripheral nerves with pre-existing deficits, such as ulnar nerve transposition and carpal tunnel release. In addition, the operative site may be adjacent to neural structures, as with total shoulder arthroplasty or fractures of the proximal humerus. The decision to perform regional anesthesia in a patient with pre-existing neurologic deficits or who is at risk for perioperative neurapraxia should be made on an individual basis after discussion with the patient and surgeon. Meticulous regional anesthetic technique with appropriate use of local anesthetic solutions and vasoconstrictors, careful patient positioning, and serial postoperative neurologic examinations may reduce the incidence of neurologic dysfunction.
Local anesthetic selection is based on the duration and degree of sensory or motor block required. Although prolonged blockade of the lower extremities interferes with ambulation and therefore delays outpatient discharge, persistent upper extremity block is not a contraindication to hospital dismissal. However, the patient should be informed of the anticipated duration of analgesia during the postoperative visit and instructed to protect the blocked extremity until block resolution.
Surgery to the Shoulder and Upper Arm
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


