INTRODUCTION
ASSESSING PAIN
To treat patients’ pain, it is vital to assess it. There are several common methods to do this, including the following:
The five-point pain scale using words, in which patients point to the word that best expresses their pain level (Fig. 14-1). However, to use this, the patient must understand each of the terms for gradations of pain. (The words in the figure are provided in several languages.)
Faces pain scales (Figs. 14-2 and 14-3), which can be used by nonverbal patients or when language difficulties exist.1
Pain Assessment for Children (Table 14-1) can be used for children <4 years old and for children who are nonverbal or noncommunicative. It provides a rough guide to their discomfort level.

FIG. 14-2.
Faces pain scale: adult. This scale can be used (a) with patients without language ability, (b) where a language barrier exists between the patient and health care provider, (c) with preverbal children, or (d) with those who are deaf. The numbers 1 to 10 on this scale correlate to those used on the other linear scales.
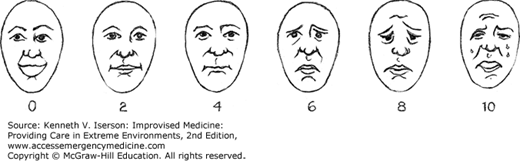
FIG. 14-3.
Faces pain scale: children. This figure may work well with children.1 Explain to the child that each face is for a person who feels happy because he has no pain (hurt) or who feels sad because he has some or a lot of pain. Ask the child to point to the face that best describes how he is feeling. The numbers correlate to those used on the other linear scales.
Face 0 is very happy because he doesn’t hurt at all.
Face 2 hurts just a little bit.
Face 4 hurts a little more.
Face 5 hurts even more.
Face 8 hurts a whole lot more.
Face 10 hurts as much as you can imagine, although you do not have to be crying to feel this bad.

| If the child is asleep, no further assessment is needed. If the child is awake, check the following: | ||
|---|---|---|
| Score | ||
| 1. Cry? | Not crying Crying | 0 1 |
| 2. Body position? | Relaxed Tense | 0 1 |
| 3. Facial expression? | Relaxed or happy Distressed | 0 1 |
| 4. Response? | Responds when spoken to No response | 0 1 |
The potential effect of analgesic treatment on pain can be assessed rapidly using intravenous (IV) drug challenges in conjunction with repeated use of the pain scales. Such evaluations can be done with minimal equipment and with commonly available medications. In addition, they can often be combined with sequential sensory neurological examinations. The two most common drugs used for this test are lidocaine and ketamine. If they significantly reduce a patient’s pain, this can indicate additional treatment options.
These are often successful, especially in treating peripheral nerve pain. The safest, especially in patients with a history of arrhythmias or seizures, is a 4-hour infusion of 2 mg/kg IV. Dilute the lidocaine in 240 mL of normal (0.9%) saline (NS) and run it at 1 mL/min. Monitor pain scores every 15 minutes. If available, use cardiac monitoring and oximetry. If the patient has a positive response (less pain) with the lidocaine infusion, additional periodic lidocaine infusions will probably be an effective analgesic. Positive response to lidocaine indicates that mexiletine (an oral medication in the same class) may be effective.2
Ketamine has successfully treated a wide variety of pain syndromes, including those that have become resistant to opioids. The method is to administer 0.15 mg/kg over 20 minutes. Diluting the ketamine in 20 mL of NS or glucose (D5W) allows administration of 1 mL/min. Monitoring and pain testing should be as with the lidocaine infusion. Terminate the infusion (positive test) if the pain scale is ≤2 out of 10. With a positive response, consider using oral ketamine. Calculate a starting dose as 10% to 20% of the amount needed to lessen the patient’s pain significantly, with a maximum adult starting dose being 100 mg/day.2 (See the “Ketamine” section in this chapter and in Chapter 17 for more information.)
TREATING PAIN
Treat pain whenever possible. An unreasonable fear of analgesia’s side effects or of addiction, coupled with minimal staff and training, may propagate “a culture of nonintervention,” in which nontreatment of pain becomes the norm. In addition, although narcotics are the gold standard for treating moderate to severe pain, many countries either ban their use outright or have so many restrictions or regulations governing their importation and use that clinicians rarely employ them.
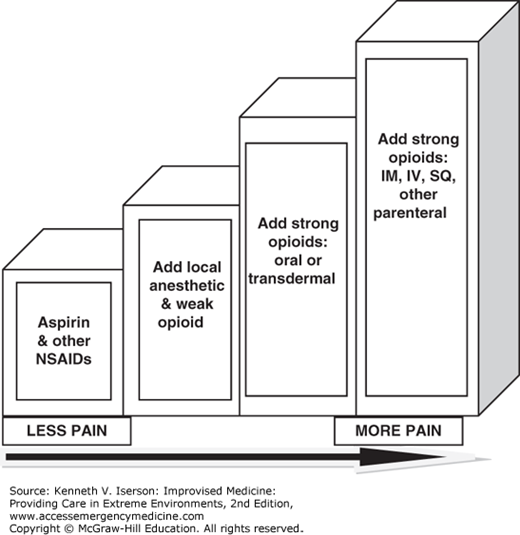
A treatment pain ladder describes an optimal treatment strategy that starts with the weakest medications and progressively increases the strength of the medication. The Wilderness Medical Society recommends using acetaminophen with a nonsteroidal anti-inflammatory drug (NSAID) as the first-line medication for acute pain in remote settings.4 If the patient has no relief, they are moved from an NSAID or another non-opioid drug to a weak opioid with or without another agent, and, finally, to strong opioids. Codeine and propoxyphene are weak opioids.5
A system that has been advocated for use with this pain ladder is “by the mouth” (use oral medications, if possible), “by the clock” (don’t wait until the pain develops and is hard to control: use the medications on a fixed schedule to avoid getting the pain), and “by the ladder” (use the progressive system).6
The World Federation of Societies of Anaesthesiologists (WFSA) Analgesic Ladder uses regional anesthesia and a limited number of analgesics in a three-step approach.3 A combination of these two methods (Fig. 14-4) represents the way clinicians should actually deliver analgesia to achieve optimal results. The type of analgesic intervention begins along the continuum, depending on the acuity, severity, and nature of the pain.
Rather than parenteral administration, whenever possible, give analgesics by mouth (po) or via the rectum in children. Avoid aspirin, because of its association with Reye’s syndrome.
If supplies are or will be limited, it helps to know which analgesics provide the most “bang for the buck.” Although clinicians most often use analgesics based on tradition, the Oxford League’s Table of Analgesic Efficacy provides some rational guidelines.
Based on published reviews, the Oxford League Table of Analgesic Efficacy (Table 14-2) lists commonly used analgesic medications (not IV) and the percentage of patients achieving at least 50% pain relief over 4 to 6 hours as compared with a placebo in randomized, double-blind, single-dose studies in patients with moderate to severe pain. Drugs were oral, unless specified. Note that commonly used medications such as tramadol, codeine (alone or in combination with paracetamol/acetaminophen, aspirin, or dextropropoxyphene), dextropropoxyphene alone, and lower doses of the listed medications were less effective in relieving pain than were many others that are commonly available.7
| Analgesic (mg) | Percentage With ≥50% Pain Relief (%) |
|---|---|
| Ibuprofen 800 | 100 |
| Piroxicam 40 | 80 |
| Ibuprofen 600 | 79 |
| Valdecoxib 40 | 73 |
| Oxycodone IR 15 | 73 |
| Valdecoxib 20 | 68 |
| Diclofenac 100 | 67 |
| Oxycodone IR 10 + acetaminophen 1000 | 67 |
| Oxycodone IR 10 + acetaminophen 650 | 66 |
| Acetaminophen (paracetamol) 1500 | 65 |
| Rofecoxib 50 | 63 |
| Diclofenac 50 | 63 |
| Piroxicam 20 | 63 |
| Bromfenac 100 | 62 |
| Aspirin 1200 | 61 |
| Acetaminophen 500 | 61 |
| Oxycodone IR 5 + paracetamol 500 | 60 |
| Naproxen 220/250 | 58 |
| Ketorolac 20 | 57 |
| Acetaminophen 1000 + codeine 60 | 57 |
| Ketorolac 60 (IM) | 56 |
| Lumiracoxib 400 | 56 |
| Ibuprofen 400 | 56 |
| Oxycodone IR 5 + paracetamol 1000 | 55 |
| Diclofenac 25 | 54 |
| Meperidine (Pethidine) 100 (IM) | 54 |
| Bromfenac 50 mg | 53 |
| Ketorolac 30 (IM) | 53 |
| Bromfenac 25 | 51 |
| Naproxen 440 | 50 |
| Ketorolac 10 | 50 |
| Morphine 10 (IM) | 50 |
Although clinicians regularly administer opioid analgesics, those may not always be available or parenteral narcotics may need to be used orally. Table 14-3 lists the equianalgesic doses when using parenteral opioids by mouth.
| Equianalgesic Dose (mg) | ||
|---|---|---|
| Opioid | Oral | Parenteral |
| Morphine | 30 | 10 |
| Fentanyl | N/A | 0.1 |
| Hydromorphone | 7.5 | 1.5 |
| Methadone | 20 (acute) 2-4 (chronic) | 10 (acute) 2-4 (chronic) |
| Oxycodone | 20 | N/A |
| Codeine | 200 | 120 |
| Meperidine | 300 (not recommended) | 75 |
| Propoxyphene | N/A | 130-200 |
UNCOMMON ANALGESICS AND ADJUVANTS
Sucrose or other sweet solutions (e.g., glucose) offer a safe and effective nonpharmacologic way to decrease pain in infants during procedures. Children achieve the greatest analgesic effect when they receive 2 mL of at least 24% sucrose ~2 minutes before the painful stimulus. The analgesic effect lasts ~4 minutes.9 These solutions are easy to administer, inexpensive (approximately US $1 per dose), have few to no adverse effects, and have been shown to decrease pain scores and crying time during painful procedures such as heel lances and immunizations.10 At least in premature infants (32-37 weeks), the combination of sucrose with nonnutritive sucking provides better pain relief than both methods separately.9
If available (~60% of UK emergency departments use it), intranasal diamorphine is a safe option that works at least as well as IV or intramuscular (IM) morphine in children with severe pain. For maximal absorption, administer it in small volumes (0.1 mL) of saline.11
Ketamine is available throughout the world as an anesthetic (see Chapter 17 for that use). Its availability combined with its effectiveness as an analgesic makes it an excellent choice for treating severe pain. Ketamine provides good analgesia when administered intramuscularly (IM), intravenously (IV), and, in much lower doses, via the oral, intranasal, transdermal, rectal, and subcutaneous routes. It has proven effective for refractory neuropathic pain, such as postherpetic neuralgia, postamputation pain, spinal ischemia, brachial plexopathy, and HIV and cancer neuropathies. It is also effective in nociceptive pain, including myofascial and ischemic pain.12,13,14,15
Subanesthetic concentrations of ketamine also provide effective analgesia for short, painful procedures, such as burn-dressing changes, radiotherapeutic procedures, bone marrow aspiration, and minor orthopedic procedures.16
Note that ketamine analgesia (1 mg/kg IV) has a pressor effect in circulatory shock and is the analgesic of choice for trauma patients in shock, especially if it is being used within 6 to 12 hours after injury. More care is needed if the patient is farther out from the injury, when it may cause hypotension. In patients with eye injuries, it may cause increased intraocular pressure at low doses.17
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


