106 Allergic Disorders
 Key Points
Key Points• Allergy refers to inappropriate responses (hypersensitivity) by the host’s immune system.
• Anaphylaxis is an acute, potentially fatal, systemic allergic reaction. Deaths in patients with anaphylaxis are caused by acute respiratory failure.
• Foods, medications, and insect stings are the most common agents causing anaphylaxis.
• Epinephrine is the first-choice medication in the treatment of anaphylaxis, with H1 and H2 antihistamines and steroids being helpful adjuncts.
• Most cases of angioedema are mediated by IgE and respond to allergic therapy. Certain forms of angioedema, however, are mediated by bradykinin and may respond to new classes of medications, the kallikrein inhibitor (ecallantide) and C1 esterase inhibitor concentrates (Cinryze, Berinert).
Allergic Disease: Allergic Rhinits, Insect Stings, Drug Allergy
Epidemiology
The prevalence of allergic disorders, including the incidence of anaphylaxis, has been increasing worldwide in the last few decades and is a topic of intensive study.1,2 Features of Western lifestyles, such as changes in infant diets, widespread use of antibiotics, smaller family size, and cleaner child care, are believed to reduce stimulatory antigenic exposure in an individual’s early years. This has led to an environment in which the immune system is dominated by a persistent allergy-prone system.3
Allergic Rhinitis
It is estimated that up to 42% of Americans suffer from some form of allergic rhinitis at any one time,4 and it has been shown to have a strong correlation with asthma. In recent studies, nearly 40% of adults with allergic rhinitis were also found to have asthma, and 80% of asthmatics demonstrated signs of rhinitis.
Insect Stings
Serious systemic reactions to insect stings are rare and occur in 1% of children and 3% of adults. Anaphylactic reactions account for approximately 50 deaths annually in the United States. There is a 2 : 1 male-to-female distribution, and adult male agricultural workers are considered the most vulnerable population. Individuals who experience large local reactions are less likely to have a systemic reaction (5% to 10%).5
Drug Allergy
A drug allergy is defined as an immune-mediated adverse response to a drug. An adverse drug reaction is defined as a noxious, unintended, or undesired response to a drug taken at a normal dose for the prevention, diagnosis, or treatment of a disease,6 and a drug side effect is an expected and known (adverse) effect of taking the drug that is not the intended therapeutic outcome. Although the true frequency is unknown, drug allergy is thought to account for approximately one third of adverse drug reactions.7 Adverse drug reactions affect 10% to 20% of hospitalized patients and more than 7% of the general population.
Pathophysiology
The immune system protects the host by distinguishing self from nonself; it tolerates the former but attacks the latter.8,9 Allergy, allergic diseases, and hypersensitivity reactions arise when our immune system reacts inappropriately to allergens with resultant harm to the host.1,2,10,11 For allergic diseases to occur, predisposed individuals need to first be exposed to an allergen through a process called sensitization.
Hypersensitivity reactions are mechanistically divided into four types of reactions according to the Gell and Combs classification system (Box 106.1). The immediate hypersensitivity reaction (type I), which is mediated by IgE, serves as the classic model of the immune response to allergen. On initial exposure to allergen, T helper 2 (TH2) cells are activated, which results in the production of an array of cytokines that exert their effects on the T cells themselves, B cells, and antigen-presenting cells. IgE is elaborated and attached to the high-affinity Fc receptor on the surface of mast cells and basophils. Fixation of allergen-specific IgE leads to a series of cellular and molecular changes that prime these cells for future exposure. On reexposure, allergen cross-links the cell-bound IgE on the surface of mast cells and basophils, thereby setting in motion a complex cascade of events that lead to the release of preformed mediators such as histamine, lipid mediators, and cytokines and subsequent activation of various inflammatory pathways. These mediators and products of secondary inflammatory pathways cause adherence and chemotaxis of inflammatory cells, increased capillary permeability, vasodilation, smooth muscle contraction, and sensory nerve stimulation. A few allergen molecules can thus cause the release of a large number of mediator molecules in a designed amplification response. Examples of type I hypersensitivity reactions include allergic rhinitis, allergic asthma, urticaria, angioedema, and anaphylaxis.
See Box 106.1, Types of Hypersensitivity, online at www.expertconsult.com.
Box 106.1 Types of Hypersensitivity
Allergens are typically carbohydrate or protein molecules (or parts of a larger molecule) that elicit an immune response.10
The inflammation that occurs in allergy is divided into three temporal phases.10 Early-phase reactions occur within minutes of exposure and are considered immediate type I hypersensitivity reactions. Late-phase reactions typically occur within 2 to 6 hours and peak 6 to 9 hours after exposure. This response is thought to be due to newly synthesized cytokines, growth factors, and chemokines, which were released more slowly than the preformed mediators primarily responsible for the early-phase reaction. This reaction often involves airway narrowing and hypersecretion of mucus in the lungs, in addition to the erythema, warmth, and pain experienced in the skin. In some individuals there is no clinical distinction between the early and late phases. Chronic allergic inflammation is the final phase in the inflammatory process. It occurs after persistent or repetitive exposure to specific allergens and results in tissue remodeling and structural changes in affected cells. Chronic allergic inflammation can further increase epithelial injury, mucus production, and thickening of airway walls.
The majority of serious sting-related reactions are caused by insects belonging to the order Hymenoptera (yellow jackets, hornets, honeybees, wasps, and fire ants).5 Their venom contains histamine, dopamine, various peptides, and protein enzymes that are either vasoactive or can elicit significant allergic reactions (IgE mediated).
Presenting Signs and Symptoms
Insect Stings (Hymenoptera Venom Allergy)
Patients with systemic allergic reactions from stings may exhibit generalized urticaria, angioedema, wheezing, stridor, anxiety, or other signs of respiratory and circulatory insufficiency. Most stings, however, cause self-limited local reactions consisting of redness, pain, and itching at the site of the sting. These reactions typically develop within minutes and usually last for a few hours. Local reactions rarely put patients at risk for future systemic reactions.5 Fire ant stings tend to produce pustulelike lesions. Local stings that result in subsequent swelling near the oropharynx (either cutaneous or deep) can cause airway compromise, and affected patients should be observed in the emergency department (ED) until the symptoms have resolved.
Differential Diagnosis and Medical Decision Making
Allergic Rhinitis
Box 106.2 lists other diagnostic considerations in patients with symptoms that may mimic allergic rhinitis.12 Patients older than 20 years should be investigated for nonallergic causes (e.g., polyps). Atopic patients with severely inflamed conjunctivae, lids, and periorbital structures should raise the possibility of atopic keratoconjunctivitis (Fig. 106.1) and vernal keratoconjunctivitis (Fig. 106.2). These two types of chronic allergic conjunctivitis have the potential to cause corneal erosions and ulcers leading to vision loss and should be managed in consultation with an ophthalmologist.
Box 106.2
Causes of Rhinorrhea and Nasal Obstruction
Modified from Greiner AN. Allergic rhinitis: impact of the disease and considerations for management. Med Clin North Am 2006;90:17–38.

Fig. 106.1 Atopic keratoconjunctivitis.
(From Baba I. Red eye—first aid at the primary level. Community Eye Health 2005;18:70–72.)
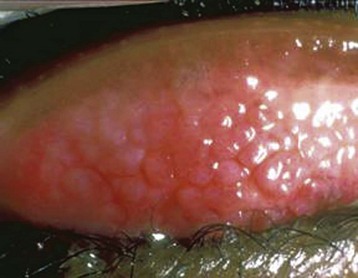
Fig. 106.2 Vernal keratoconjunctivitis.
Notice the lumpy appearance on the conjunctivae.
(From Yorston D, Zondervan M. Red eye picture quiz. Community Eye Health 2005;18:72–78.)
Drug Allergy
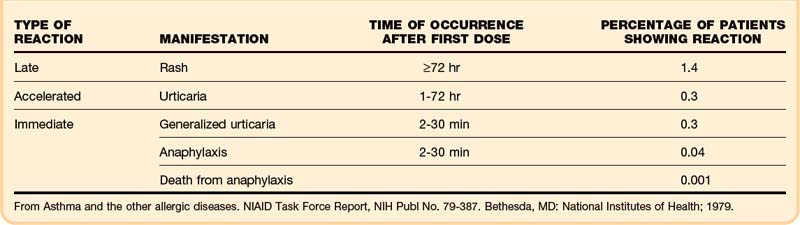
Studies show that 4.4% of patients whose penicillin allergy history was confirmed by a positive skin test experienced an allergic reaction to cephalosporins.13 Only 10% to 20% of patients who report a history of penicillin allergy are truly allergic when assessed by skin testing.14 Although the overall risk for a cross-allergic reaction to cephalosporins in patients with a history of a penicillin allergy is low, the use of cephalosporins requires weighing the risks versus benefits based on an informed discussion between the patient and treating physician. Table 106.1 shows the incidence of allergic reactions to penicillin.15 Some factors can transiently cause T cells to falsely identify the penicillin epitope as being allergic. For example, in up to half (50%) of patients with mononucleosis, a maculopapular rash develops after taking amoxicillin. These same patients often have no adverse drug reaction on subsequent challenge with amoxicillin at a later time. Penicillin allergy should not be diagnosed in such patients.
Treatment
Allergic Rhinitis
Oral second-generation H1 blockers (loratadine, fexofenadine), oral decongestants (pseudoephedrine), and nasal decongestants (oxymetazoline, phenylephrine) can be used for mild, intermittent symptoms.16 Moderate to severe and persistent nasal symptoms may require the addition of intranasal steroid (fluticasone, triamcinolone, budesonide), or chromone derivative such as cromoglycate and nedocromil. An intraocular antihistamine (olopatadine), intraocular chromone, or intraocular ketorolac can be used for ocular allergies, including conjunctivitis.17
Drug Allergy
The most prudent approach in managing possible drug allergy–related complaints in the ED is to discontinue use of the suspect medication or medications, treat the allergic symptoms, and prescribe a suitable alternative drug or drugs. Severe symptoms should be treated in the same way as anaphylaxis (see Box 106.8). Patients with Stevens-Johnson syndrome and toxic epidermal necrolysis require a multidisciplinary approach that includes an intensivist, burn surgeon, and endocrinologist or allergist. For minor allergic drug reactions, H1 antihistamines can be prescribed for itching, flushing, and rash. Steroids are reserved for serious or extensive drug reactions.
Urticaria
Epidemiology
Urticaria (hives) is a fairly common reaction that affects approximately 20% of the population at some point in their lifetime.18 It has numerous different underlying causes and consists of several different types and subtypes. Spontaneous urticaria is broadly divided into acute (<6 weeks) and chronic (≥6 weeks) forms, with the latter representing approximately 10% to 20% of cases.
Pathophysiology
The classic wheal lesions associated with urticaria are the result of edema within the mid and upper dermal layers of the skin. Dilation of lymphatic vessels and capillary venules allows extravasation of protein-rich fluid into the surrounding tissue. This complex inflammatory process involves a variable mixture of macrophages, T cells, neutrophils, eosinophils, and mast cells.19
Presenting Signs and Symptoms
Patients with urticaria usually have hives of variable duration and location.20,21 Urticarial lesions are pruritic, erythematous, raised rashes that blanch on palpation. The lesions are typically round or oval with serpiginous borders, but they may vary in color, size, and shape (Fig. 106.3). They may be localized or appear throughout the body, but there is a slight predilection for the trunk, hands, feet, lips, tongue, and ears. Urticaria usually starts with erythema (flare) as a result of capillary vasodilation in the superficial layer of the dermis. As the protein-rich fluid extravasates into surrounding tissue, it evolves into raised wheals and may change from red to white. A history of pruritic red rash that changes in size and shape, with extension and regression over a period of hours or days, favors the diagnosis of urticaria.








