199 Addiction
 Key Points
Key Points• Drug abuse and alcohol abuse irrevocably change brain physiology; addiction represents a brain disorder.
• The acute manifestations of substance abuse and dependency arise from drug-specific patterns of intoxication and withdrawal.
• Acute pharmacologic detoxification is accomplished through the administration of a long-acting medication in the same category as the drug of dependence, thereby blocking withdrawal symptoms.
• Anticraving medications are psychotropic agents that reduce the desire for drugs or alcohol in detoxified patients and prevent relapse into compulsive substance abuse.
Scope, Epidemiology, and Definitions
From several viewpoints the problem is vast. Regarding alcohol, the Centers for Disease Control and Prevention reports that approximately 79,000 deaths are attributable to excessive alcohol use annually in the United States, which makes it the third leading lifestyle-related cause of death for the nation. In addition, excessive alcohol use accounts for 2.3 million years of potential life lost annually—an average of about 30 years of potential life lost for each death.1 Concerning drugs, the Substance Abuse and Mental Services Administration of the U.S. Department of Health and Human Services reported that in 2009, 21.8 million Americans used an illegal drug during the month before the survey, which represents 8.7% of the population aged 12 years or older. Illegal drugs include marijuana or hashish, cocaine (including crack cocaine), heroin, hallucinogens, inhalants, and nonmedical use of prescription-type psychotherapeutics.2
Many of those abusing or dependent on alcohol or drugs, or both, disproportionately consume public health care resources, particularly emergency services. Between 1992 and 2000, alcohol-related visits to U.S. emergency departments (EDs) averaged 76 million per year, which accounted for 7.9% of the total ED visits.3 The Drug Abuse and Warning Network reported that in 2007, 1.9 million ED visits were associated with drug misuse or abuse. Although the overall number of ED visits attributable to drug misuse and abuse was stable from 2004 to 2007, ED visits involving nonmedical use of pharmaceuticals with no other drug involvement rose significantly (73%), as did the nonmedical use of pharmaceuticals with alcohol (36%).4
The societal burdens of substance abuse extend well beyond EDs. The U.S. Office of National Drug Control Policy reported that incarcerated offenders were often under the influence of drugs when they committed their offenses and that offenders often commit crimes to support their drug habit. In addition, trafficking in illicit drugs tends to be associated with the commission of particularly violent crimes.5
The cumulative economic cost of substance abuse is astounding. In 1998, alcohol abuse in the United States cost approximately $185 billion, with 47% of this cost simply being due to lost productivity at work.6 The same year, drug abuse in the United States cost $143 billion.7 When adjusted for 2010 dollars, abuse of both drugs and alcohol costs the nation $440 billion—the equivalent of 80% of all revenue raised to fund public education for grades prekindergarten through 12.8 Substance abuse is as much a public crisis for our nation as it is a personal crisis for the addict.
With substance abuse, adverse consequences occur but the pattern has not yet deteriorated into a state of dependence. More specifically, the American Psychiatric Association defines substance abuse as “a maladaptive pattern of substance use” revealed by the recurrent and significant consequences arising from repeated use of the substance: failure to fulfill major role obligations, recurrent use in situations in which it is physically hazardous, multiple substance-related legal problems, and recurrent social and interpersonal problems9 (Box 199.1). Although the consequences of use are significant, some degree of control is present.
Box 199.1
Criteria for Substance Abuse
A. A maladaptive pattern of substance use leading to clinically significant impairment or distress, as manifested by one (or more) of the following occurring within a 12-month period:
B. The symptoms have never met the criteria for substance dependence for this class of substance.
From First MB, Frances A, Pincus HA. Substance-related disorders. In: DSM-IV-TR guidebook. Washington, DC: American Psychiatric Publishing; 2004.
In contrast, substance dependence is defined as severe impairment or absence of control. Use is compulsive and occurs under the ever-present threats of tolerance and withdrawal. As stated earlier, the American Psychiatric Association more specifically defines substance dependence as a cluster of cognitive, behavioral, and physiologic symptoms indicating continued use of the substance despite significant substance-related problems9 (Box 199.2).
Box 199.2
Criteria for Substance Dependence
1. Tolerance, as defined by either of the following:
2. Withdrawal, as manifested by either of the following:
3. The substance is often taken in larger amounts or over a longer period than was intended.
4. There is a persistent desire or unsuccessful efforts to cut down or control substance use.
5. A great deal of time is spent in activities necessary to obtain the substance (e.g., visiting multiple doctors, driving long distances), use the substance (e.g., chain smoking), or recover from its effects.
6. Important social, occupational, or recreational activities are given up or reduced because of substance use.
7. The substance use is continued despite knowledge of having a persistent or recurrent physical or psychologic problem that is likely to have been caused or exacerbated by the substance (e.g., current cocaine use despite recognition of cocaine-induced depression, continued drinking despite recognition that an ulcer was made worse by alcohol consumption).
From First MB, Frances A, Pincus HA. Substance-related disorders. In: DSM-IV-TR guidebook. Washington, DC: American Psychiatric Publishing; 2004.
Tolerance is reflected by the “need for increasing amounts of the substance to achieve intoxication or desired effect … or diminished effect with continued use of the same amount of the substance.”9
Withdrawal is a physiologic response manifested by the characteristic “withdrawal” syndrome for the particular substance or use of the same or a closely related substance to relieve or avoid such symptoms.9
Pathophysiology and Anatomy
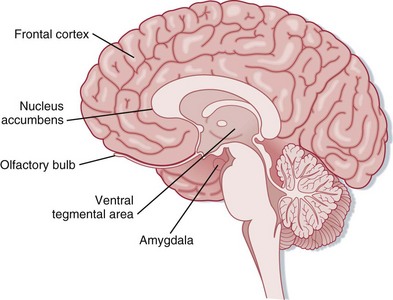
Addiction changes brain physiology, thus prompting designation of this condition as a brain disorder.10 Addictive substances alter multiple neurotransmitter pathways within the brain, including N-methyl-D-aspartate (NMDA) and γ-aminobutyric acid (GABA) receptors, as well as the endogenous opioid, serotonin, and dopamine systems.11 Changes particularly occur within the mesolimbic system of the brain. Projecting from the ventral tegmental area to the nucleus accumbens, olfactory tubercle, frontal cortex, and amygdala, the mesolimbic system is regarded as the “reward center” of the brain12 (Fig. 199.1). These neurocircuits presumably evolved to reward survival-enhancing behavior, including productive familial and social interactions, reproduction, and other such behavior. Some suggest that mesolimbic dopamine is a direct mediator of reward, whereas others emphasize that dopamine signals an interest in reward or the expectation that reward is forthcoming. Either way, evidence suggests that the common reinforcing and incentive effects of addictive substances are substantially mediated by increasing extracellular dopamine within the mesolimbic system. On an elementary level, this drug-induced efflux of dopamine is pleasurable.10
See Figure 199.1, Mesolimbic Dopaminergic System, online at www.expertconsult.com
As addicts and clinicians mutually recognize, artificially inducing the mesolimbic system with drugs and alcohol for these pleasant effects is accompanied by grave shortcomings. Neurochemical pleasure circuits, overwhelmed by excessive stimulation, adapt by desensitizing.13 Evaluation by multiple disciplines, including anatomic, behavioral, biochemical, and electrophysiologic studies, commonly shows that dopamine neurons function insufficiently in addicts. A hypodopaminergic state develops.10 The dopamine deficiency associated with acute withdrawal is manifested clinically as acute dysphoria, depression, irritability, and anxiety. Neurochemically, baseline levels of the “reward” neurotransmitters are depressed.12 The traditional social and behavioral stimulants of the mesolimbic system that function effectively in the nonaddictive state, such as family and positive affirmation from work or friends, become inadequate to generate a significant perception of pleasure. Drugs and alcohol are the sole stimuli sufficient to activate the impaired mesolimbic neurocircuits and generate pleasure.13 Yet even though the baseline mesolimbic system remains hypodopaminergic in addicts, the system remains hyperresponsive to abused drugs and alcohol, thereby conferring long-lasting vulnerability even after extensive periods of abstinence.10 The most promising avenues of treatment for addicts are pharmacologic agents aimed at restoring these dopaminergic neurocircuits.10
Not all individuals are equally susceptible. Those with risk-taking and novelty-seeking traits favor the use of addictive drugs. Psychiatric conditions, in particular, schizophrenia, bipolar disorder, and attention-deficit/hyperactivity disorder, are associated with increased risk for substance abuse and dependency. A dual diagnosis of substance abuse and mental disorder has especially unfavorable implications for both management and outcome.14
Genetic factors clearly increase the risk for addiction. First-degree relatives of alcoholics (e.g., parents, siblings, children) have a threefold to fourfold greater prevalence of alcohol abuse than the general population does.15 Men whose parents were alcoholics have an increased likelihood for alcoholism even when adopted at birth and raised by nonalcoholic parents.14 Genetic factors, as revealed by studies in identical twins, account for approximately half of the risk for alcohol abuse.15
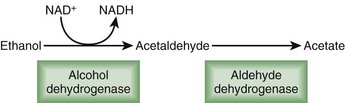
Some of this genetic predilection for addiction is expressed through enzymatic variants. For instance, highly active forms of aldehyde dehydrogenase increase alcohol metabolism and decrease the negative side effects of alcohol intake, thereby enhancing consumption and addiction (Fig. 199.2). In contrast, less active variants of aldehyde dehydrogenase (i.e., the ALDH2*2 allele initially detected in eastern Asian populations) allow accumulation of acetaldehyde, the toxic intermediary by-product of alcohol metabolism. Sensitivity to alcohol increases with a subsequent reduction in the rates of alcoholism.16 Genetic influence is also expressed through neurotransmitter variants. Neuropeptide Y, a 36–amino acid peptide neurotransmitter, regulates appetite, anxiety, and reward. A functional Lue7Pro polymorphism in the neuropeptide Y gene increases the risk for alcohol dependence by 7.3%, primarily in European Americans.17 Although the initial use of a drug or alcohol is a willful act, for those predisposed to abuse or dependency, some if not most of what follows is progressively beyond their control.
Presenting Signs and Symptoms
Acute intoxication with central nervous system depressants—alcohol, sedatives, hypnotics, and anxiolytics—is characterized by dysfunctional behavioral and neurologic changes. Individuals suffer mood swings and impaired social or occupational functioning. Poor judgment prevails, often reflected by inappropriate sexual or aggressive behavior. Neurologic dysfunction occurs along a clinical spectrum determined by the degree of intoxication and ranges from slurred speech, incoordination, and unsteady gait to impairment of memory and attention, stupor, and coma (Box 199.3




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


