104 Acute Pancreatitis
The term acute pancreatitis describes a wide spectrum of disease ranging from a mild edematous form of acute pancreatitis to severe acute necrotizing pancreatitis. Acute pancreatitis is the third most common gastrointestinal disease requiring hospitalization in the United States and accounts for annual costs of more than $2 billion.1,2 The mild form of acute pancreatitis is a self-limited disease associated with little or no distant organ dysfunction; it has a mortality rate of less than 1% and usually resolves in 3 to 4 days. Patients with this form of acute pancreatitis rarely need intensive care unit (ICU) therapy or pancreatic surgery. Although most (80%) patients with acute pancreatitis have mild disease, 10% to 15% develop the systemic inflammatory response syndrome (SIRS) and run a fulminant clinical course leading to pancreatic necrosis and multisystem organ injury.3–5 The mortality rate for severe acute pancreatitis is 15% to 30%, whereas the overall mortality rate for all patients presenting with acute pancreatitis is less than 5%.4,5 The natural course of severe acute pancreatitis occurs in two phases. The first 7 to 14 days of this disease process are characterized by SIRS and resulting end-organ dysfunction. Inflammatory mediators are released into the systemic circulation, and patients manifest signs and symptoms of cardiorespiratory and renal failure.6 Pancreatic infection is uncommon during this early phase of acute pancreatitis and SIRS, but bacteremia and pneumonia have been identified at a median of 7 days.7 Attempts to modify the course of the disease by instituting therapy with protease inhibitors, octreotide, or platelet-activating factor receptor antagonists have been unsuccessful.8–10
Since the 1980s, the morbidity and mortality associated with acute pancreatitis have decreased substantially.11–14 The reasons for the decrease in mortality in severe acute pancreatitis are uncertain but may reflect improved critical care services and better strategies for surgical management. In general, mortality from severe acute pancreatitis is related to infection.13,14 Infection of the necrotic pancreas (and associated tissues) typically develops in the second and third weeks of the disease and is reported to occur in 40% to 70% of patients with pancreatic necrosis.7,13,14 Multiple organ system dysfunction syndrome is the main life-threatening complication, and mortality rates of 50% have been reported.15 Infected necrosis is the most important risk factor for death secondary to necrotizing pancreatitis.13–16 Prevention, diagnosis, and optimal treatment of infection in severe acute pancreatitis are crucial for improving outcome for patients with this disease.
This chapter discusses the etiology, pathophysiology, severity and staging, and management of patients with severe acute pancreatitis. Chronic pancreatitis is not discussed in this chapter. Several authors and/or societies have proposed guidelines and protocols for management of severe acute pancreatitis.4,14,17–19
 Etiology and Epidemiology
Etiology and Epidemiology
In 2001 in California, the rate of hospital admission with an initial attack of acute pancreatitis was 44 per 100,000 per year, an increase of more than 32% over the decade of the study. Overall rates of hospitalization in the Unites States over the last 20 years has increased from 40 per 100,000 to 80 per 100,000 and included both sexes and all age groups.20 The increasing incidence of acute pancreatitis is believed to be related to increases in alcohol consumption and gallstone disease in some societies. Acute pancreatitis is slightly more common in men than in women, with a male-to-female ratio of 1 : 1.2 to 1 : 1.5. Predisposing factors related to race have not been identified, but both hospitalization rates and emergency department visits for patients diagnosed with acute pancreatitis are higher for blacks than for whites. Pancreatitis can occur in any age group, but cases in the very young (<3 years) are likely to be related to a systemic disease such as hemolytic uremic syndrome or cystic fibrosis. On the other hand, alcohol-related acute pancreatitis has a peak incidence between 45 and 55 years of age, with a gradual decline thereafter. Gallstone pancreatitis can occur in any age group, but its frequency increases with age. Biliary pancreatitis is more common in women, and alcohol-related acute pancreatitis is more common in men.
Understanding the etiology of a particular case of pancreatitis is important; evaluation and treatment depend to some extent on the predisposing disease process.6,17 Gallstones are the leading cause of acute pancreatitis in developed countries and account for 45% of all cases. A biliary etiology should be suspected in female patients older than age 40 with a serum alanine aminotransferase level greater than three times the upper reference limit. Gallstone pancreatitis is the commonest form of pancreatitis in older patients. Since the frequency of gallstones increases with age, gallstones should be suspected in elderly patients.
Alcohol abuse typically accounts for about 35% of cases of acute pancreatitis; however, it is unclear whether acute alcoholic pancreatitis ever arises in the absence of chronic injury to the gland.21 Infrequent, but not rare, causes of pancreatitis include drug reactions (usually idiosyncratic), pancreatic and ampullary tumors, hypertriglyceridemia, hypercalcemia (almost always secondary to hyperparathyroidism), hypothermia, congenital abnormalities of the biliary or pancreatic duct (e.g., choledochal cyst), trauma (including acute pancreatitis after endoscopic retrograde cholangiopancreatography), and infectious or parasitic organisms. Rare causes include bites of certain spiders, scorpions, and the Gila monster lizard. Unidentified causes are termed idiopathic. The roles of sphincter of Oddi dysfunction, pancreas divisum, and bile crystals or sludge in the development of acute pancreatitis are less clear.20
 Pathogenesis and Genetic Susceptibility
Pathogenesis and Genetic Susceptibility
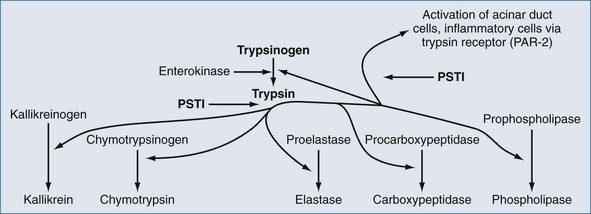
Regardless of the actual underlying cause, pancreatitis is an inflammatory process that can initiate SIRS.6 In spite of much investigation into the molecular pathogenesis of acute pancreatitis, the exact intracellular mechanisms initiating and accelerating pancreatitis are not completely understood. Three phenotypic responses occur in the acinar cell in the early phases of acute pancreatitis22,23: changes in secretions, intracellular activation of proteases, and generation of inflammatory mediators. Shortly after an appropriate stimulus, secretions are released from the apical cells into the pancreatic duct. This process entails exocytotic fusion of zymogen granules with the apical plasma membrane; the granules do not fuse with the basolateral membrane. However during acute pancreatitis, there is (1) markedly decreased apical secretion from the acinar cell, (2) disruption of the paracellular barrier in the pancreatic duct with leakage of contents into the paracellular space, and (3) redirection of secretion from zymogen granules from the apical pole to the basolateral regions of the acinar cell. Inappropriate activation of the proteolytic enzyme, trypsin, is thought to be the initial step in the development of acute pancreatitis. Trypsinogen activation is promotion by cationic trypsinogen mutations (PRSS1+), active trypsin, high calcium ion concentration, and low pH. Calcium levels are regulated in part by calcium-sensing receptors (CASR) and dysregulated by ethanol.22,23 Degradation of active trypsin is blocked by high calcium ion concentration. If trypsin in active within the pancreas, inflammation results and this up-regulates serine protease inhibitor Kazak 1 (SPINK1), which further blocks activation of trypsinogen.22 Trypsin also activates cells via the trypsin receptor, also known as protease-activated receptor 2 (PAR-2) (Figure 104-1).22 Pancreatic acinar and duct cells abundantly express PAR-2. Trypsin activity in the pancreas is controlled mainly by the pancreatic secretory trypsin inhibitor (PSTI), also called serine protease inhibitor Kazal type 1 (SPINK1).22 PSTI is synthesized in pancreas acinar cells and acts as a potent natural inhibitor of trypsin. Normally when trypsinogen is cleaved to release trypsin in the pancreas, PSTI immediately binds to the enzyme to prevent further activation of additional pancreatic enzymes. PSTI also blocks further activation of pancreatic cells via the trypsin receptor, PAR-2.
Several additional protective systems prevent pancreatic autodigestion by trypsin, and the genetic expression of these systems may contribute to the risk of developing acute pancreatitis or modulate the severity of the disease when it occurs. Trypsin-activated trypsinlike enzymes such as mesotrypsin degrade trypsinogen. Bicarbonate-rich pancreatic secretions are affected by abnormal expression of the cystic fibrosis transmembrane conductance receptor. A mutation in SPINK1, N34S, has been reported in people with familial pancreatitis,24 in children with idiopathic chronic pancreatitis,25,26 and in 2% of the control population.26 Because these mutations in SPINK1 are much more common than pancreatitis, this mutation probably is a disease modifier rather than a causative factor underlying the development of acute pancreatitis.
Genetic linkage and candidate gene studies have identified six pancreas-targeting factors that are associated with changes in susceptibility to acute and/or chronic pancreatitis, including cationic trypsinogen (PRSS1), anionic trypsinogen (PRSS2), serine protease inhibitor Kazal 1 (SPINK1), cy regulator (CFTR), chymotrypsinogen C (CTRC) and calcium-sensing receptor (CASR).22
 Diagnosis
Diagnosis
The diagnosis of acute pancreatitis is relatively straightforward when acute upper abdominal pain and tenderness, nausea, vomiting, and hyperamylasemia or hyperlipasemia are present.27 These clinical and biochemical signs are nonspecific, however, and can be present in many other acute intraabdominal conditions such as acute perforation of a hollow organ or mesenteric infarction. Many cases of acute pancreatitis still are diagnosed at autopsy. The diagnosis of acute pancreatitis can be particularly difficult in postoperative patients. Acute pancreatitis also can be hard to diagnose in patients receiving drugs for sedation and patients who are hypothermic or unable to complain of abdominal pain. The Cullen sign and the Grey Turner sign (periumbilical and flank bruising, respectively) are rare and can be present with any disease associated with retroperitoneal hemorrhage. Although hyperamylasemia is common in patients with acute pancreatitis, normal circulating amylase levels are present in 10% to 20% of all cases of acute pancreatitis. Normal serum amylase concentrations are seen predominantly in acute pancreatitis secondary to hyperlipidemia, acute exacerbations of chronic pancreatitis, and late in the course of acute pancreatitis.28 Advantages of serum amylase determination include its technical simplicity, wide availability, and sensitivity.29 This diagnostic test is plagued by low specificity, however. Serum lipase concentration increases within 4 to 8 hours of the onset of acute pancreatitis, peaks at 24 hours, and returns to normal after 8 to 14 days.29 The major advantage of serum lipase determination as a diagnostic test is its excellent sensitivity in acute alcoholic pancreatitis. Measurement of serum lipase activity also is valuable when patients present to an emergency department days after the onset of the disease, because serum lipase levels remain elevated longer than amylase levels.29 Although serum lipase formerly was believed to be a specific marker for acute pancreatitis, increased circulating levels of serum lipase can occur in many other diseases. Simultaneous estimation of amylase and lipase levels does not improve accuracy.29 Other pancreatic enzymes such as P-isoamylase, macroamylases, immunoreactive trypsinogen, and elastase generally are not considered useful for making the diagnosis of acute pancreatitis.
 Severity and Scoring
Severity and Scoring
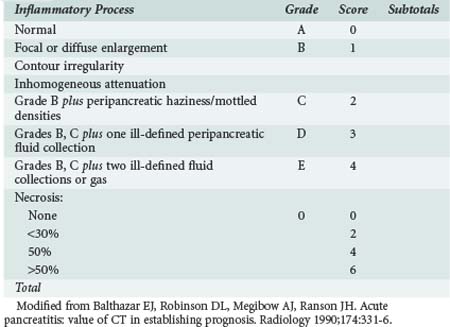
Prediction of the severity of the disease at the time of admission can be difficult, and patients can appear clinically well at admission but clinically deteriorate within 48 hours. Several different prognostic scoring systems with clinical, laboratory, and radiologic criteria have been proposed, yet none of the proposed scoring systems have a high sensitivity, specificity, positive predictive value, or negative likelihood ratio, and frequent clinical assessment is essential for identifying patients with severe disease.30 Ranson’s criteria (Table 104-1),31 the Imrie32 (Glasgow) score, the Acute Physiologic and Chronic Health Evaluation (APACHE) II and III scores,33 the simplified acute physiology score, and Balthazar’s computed tomography (CT) index (Table 104-2)34–36 are the most popular scoring systems and often are used to determine the need for admission to an ICU. Ranson’s criteria are based on 11 prognostic signs present at presentation and 48 hours later.31 A meta-analysis of studies using the Ranson criteria reported the following with regard to predicting severe acute pancreatitis (SAP): sensitivity, 74%: specificity, 77%; positive predictive value, 49%; and negative predictive value, 91%.30 The Glasgow (Imrie) severity score system collects data on 9 variables at admission but is not complete until 48 hours after admission. Many institutions routinely utilize the APACHE scoring system for all patients admitted to the ICU.33 Patients with SAP and an APACHE II score above 8 have severe disease and are likely to develop organ failure. Key statistical parameters related to APACHE II score of above 7 and the prediction of SAP are as follows: sensitivity, 65%; specificity, 76%; positive predictive value, 43%; and negative predictive value, 89%. Balthazar’s CT index34–36 uses both fluid collections and amount of pancreatic necrosis to predict outcome. A recent international group of experts concluded that an additional group of patients should be identified: those with moderately severe acute pancreatitis (MSAP).37 This is a large group of patients who meet the Atlanta classification of severe disease but do not develop organ failure. Patients in the MSAP group often develop local complications and often have long hospitalizations with significant morbidity but without mortality. In a strategy to identify those patients who will not need ICU care, Lankish et al. proposed and validated a “harmless acute pancreatitis score (HAPS).” Using this scoring system, 98% of 204 patients were correctly identified as having non-severe disease within 30 minutes of presentation.38 These simple measures included rebound or guarding on clinical examination, hematocrit greater than 43% in men and greater than 39.6 in women, and serum creatinine concentration above 2 mg/dL. Imamura and colleagues have recently proposed a simplified grading of early CT scans based on the presence or loss of enhancement of the renal rim fat. This simple assessment compared favorably with all the commonly used scoring systems.39
TABLE 104-1 Ranson’s Criteria for Patients with Non–Gallstone-Associated Pancreatitis
| At Presentation | During Initial 48 Hours |
|---|---|
| Age > 55 years | Hematocrit fall > 10% |
| White blood cell count > 16,000/µL | Blood urea nitrogen > 5 mg/dL |
| Blood glucose > 200 mg/dL | Serum calcium < 8 mg/dL |
| Serum alanine transferase > 250 U/dL | Arterial PO2 < 60 mm Hg |
| Serum lactate dehydrogenase > 350 IU | Base deficit > 4 mEq/L |
| Estimated fluid sequestration > 6 L |
Modified from Blamey SL, Imrie CW, O’Neill J, Gilmour WH, Carter DC. Prognostic factors in acute pancreatitis. Gut 1984;25:1340-6.
Many investigators have studied and proposed a variety of serum biomarkers as predictors of the severity and prognosis of acute pancreatitis.40–42 High circulating levels of C-reactive protein (CRP) (cutoff 150 mg/L) are associated with pancreatic necrosis, but there is a 48-hour latency before CRP increases, limiting its utility as an early predictor. This marker has a sensitivity and specificity of 80%. Although not ideal predictors of severity, serum concentrations of procalcitonin and interleukins (IL) 6 and 8 have some predictive value.40–42 Certain urinary markers also have some predictive value. While not used extensively clinically at the current time, procalcitonin appears to offer the greatest promise. Serum procalcitonin levels higher than 3.8 ng/mL accurately predict later organ dysfunction (sensitivity, 79%; specificity, 93%).42
The scoring systems mentioned help quantify the degree of illness, but it is essential that clinicians identify patients with impending or actual organ failure. Patients with signs of SIRS are especially at risk for further organ dysfunction.45 In a review of 259 patients with acute pancreatitis, mortality was significantly higher in patients who developed or had persistent SIRS at 48 hours (25.4%) than in patients who had transient SIRS (8%) or no SIRS in the first 48 hours (0.7%).37
An update of the Atlanta Classification system for severity of acute pancreatitis is expected soon; the system developed at the initial consensus meeting in 1992 has allowed comparisons among clinical trials and different treatment strategies.36 It defined SAP by its association with organ failure, local complications such as necrosis, abscess, or pseudocyst, or both. By consensus, the Atlanta Classification also defined SAP based upon the presence of ≥3 of Ranson’s criteria or an APACHE II score ≥ 8. Most often, SAP is a clinical expression of the development of pancreatic necrosis. Less commonly, patients with interstitial (edematous) pancreatitis can present with SAP. In addition to the previously proposed scoring systems, there is another very simple scoring system termed the Panc 3 Score.46 Three findings—hematocrit over 44 mg/dL, body mass index above 30 kg/m2, and a pleural effusion on chest x-ray—were the most sensitive predictors of overall severity. In the validation set of data, when all three of these findings were present and the pretest probability of pancreatitis was between 12% and 25%, the posttest likelihood of severe disease was 99%.43
Serum concentrations of CRP, neutrophil elastase, pancreatitis-associated peptide, IL-6, IL-8, IL-1, IL-10, and soluble tumor necrosis factor (TNF) receptors might be useful for the early prediction of severity of disease in acute pancreatitis.40 Circulating CRP concentration is an independent predictor of outcome in acute pancreatitis, but it is not predictive of severity at presentation.44 Laboratory tests also can be used for severity stratification; serum IL-6 concentration greater than 2.7 pg/mL within 48 hours from disease onset and a serum CRP level above 150 mg/L at 48 hours after pain onset can both be used. A recent meta-analysis of the role of procalcitonin in the identification of patients with SAP suggested that the test has a sensitivity of 0.72 for the diagnosis, a specificity of 0.86, and an area under the curve of 0.87, but the studies showed a fair amount of heterogeneity.42 Trypsinogen-2 can be measured via a simple serum immunofluorometric assay or urine dipstick assay, using a threshold of 50 µg/L.41
 Imaging
Imaging
Ultrasonography And Endoscopic Ultrasonography
Ultrasonography should be considered as an initial test in all patients with pancreatitis, especially if gallstones are suspected.5,17,19 By aiding in the diagnosis of gallstones, common bile duct stones, common bile duct dilation, and free peritoneal fluid, ultrasonography can be useful for determining the cause of pancreatitis.47 Ultrasonography currently has little role in the grading of severity of acute pancreatitis or determination of extent of pancreatic necrosis. However, this situation may change because of the evolution of contrast-enhanced ultrasonography. This technique employs microbubbles as a blood-pool contrast medium to allow visualization of tissue vascularization. Early in the course of pancreatitis, inflammation is associated with hyperemia. Later in the course of severe disease, contrast-enhanced ultrasonography can reveal confluent necrotic areas of devitalized pancreatic tissue.48 The value of ultrasonography is compromised by overlying bowel gas in at least 25% to 30% of cases.
Endoscopic ultrasonography (EUS) combines ultrasonography and endoscopic evaluation. It is less invasive than endoscopic retrograde cholangiopancreatography (ERCP) and has been shown to be clinically useful in diagnosing acute pancreatitis and choledocholithiasis.47 Endoscopic ultrasonography may be useful when CT and ultrasonography fail to show common bile duct stones. Endoscopic ultrasonography also may be useful for selecting patients who might benefit from endoscopic retrograde cholangiopancreatography and early stone extraction. Petrov et al. reviewed studies of patients randomized to EUS-guided ERCP (n = 213) versus ERCP alone (n = 210). These authors showed that ERCP could be avoided in 67.1% patients when EUS failed to identify gallstones.47 The use of EUS significantly reduced the risk of overall complications [relative risk (RR) 0.35, 95% confidence interval (CI) 0.20-0.62] and post-ERCP pancreatitis (RR 0.21, 95% CI 0.06-0.83). One additional advantage of endoscopic ultrasonography is that it can be performed in pregnant women, patients with metallic implants, and patients who are too unstable to be transported out of the ICU.47
Computed Tomography
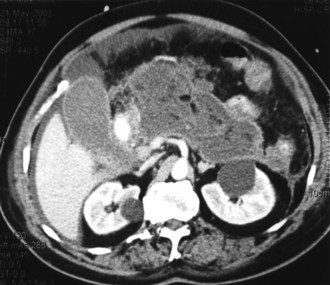
Contrast-enhanced CT is considered the gold standard for diagnosing pancreatic necrosis and peripancreatic collections and for grading acute pancreatitis (see Table 104-2).34–36 Necrosis is detected by CT as focal or diffuse areas of diminished pancreatic parenchymal contrast enhancement (<50 Hounsfield units). The accuracy of this test is greater than 90%. CT findings of acute pancreatitis include diffuse or segmental enlargement of the pancreas (interstitial edema), irregularity of the contour of the pancreas with obliteration of the peripancreatic fat planes, heterogeneous appearance with areas of decreased density within the pancreas, and variable ill-defined fluid collections (Figures 104-2 and 104-3).34–36 The Balthazar index ranges from 0 to 10 and is obtained by adding the points attributed to the extent of the inflammatory process to the volume of pancreatic necrosis. Although CT findings correlate with clinical course and severity of patients with acute pancreatitis,36 it is not necessary to obtain this study in patients with mild pancreatitis. In a recent Dutch observational study of 166 patients admitted with acute pancreatitis, early CT (within 4 days of admission) was performed in 47% of all patients. However, only 18 of the 166 patients had severe disease, and 11 eventually developed pancreatic necrosis. No changes in clinical management resulted from obtaining early CT scans. These data suggest that the use of early CT, especially in patients with mild disease, should be discouraged.49 CT can be helpful when the diagnosis is in doubt or when complications of pancreatitis may be developing. In general, contrast-enhanced CT scans should not be performed during the first 72 hours of the disease, because necrosis may not be fully established until after 96 hours, and there have been isolated reports of intravenous (IV) contrast material causing derangements of the pancreatic microcirculation.49 Contrast administration also can trigger or exacerbate renal insufficiency.

Endoscopic Retrograde Cholangiopancreatography
Endoscopic retrograde cholangiopancreatography is an effective means for treating common bile duct stones.47 Endoscopic retrograde cholangiopancreatography is not indicated for the management of mild pancreatitis or nonbiliary pancreatitis, and its overall use in patients with acute pancreatitis continues to be debated.50–58 Guidelines from England, Japan, and the United States indicate that ERCP is indicated in the management of patients with biliary pancreatitis and biliary obstruction or cholangitis.17–1952 There remains controversy regarding the role of ERCP for the management of patients with biliary pancreatitis but without bile duct obstruction. Five clinical trials have sought to determine whether ERCP plus sphincterotomy or conservative management is more appropriate for patients with acute pancreatitis.53–57 In a study of 121 patients randomized to ERCP or conservative treatment within 72 hours of onset, there was a significant reduction in morbidity (17% versus 34%; P=.03) but no significant difference in mortality (2% versus 8%; P=.23).53 The differences in morbidity seen in this trial cannot be explained by differences in the severity of pancreatitis between the two groups.53
In another study that enrolled 195 patients, ERCP performed within 24 hours was compared with conservative therapy. ERCP was associated with a significant reduction in morbidity (biliary sepsis; P = .001) without a significant reduction in mortality (five deaths with ERCP versus nine deaths with conservative treatment).54 Included in this study were patients with nonbiliary pancreatitis such as alcohol-related and parasite-related disease. In another trial with a similar design, 280 patients were randomized to receive ERCP within 24 hours or conservative treatment55; 75 of the 178 patients in the ERCP arm had impacted biliary stones. This study is the only one that showed a significant reduction in morbidity and mortality.
The study by Folsch and colleagues56 was a multicenter trial of ERCP versus conservative management. Patients with biliary sepsis and obstruction were excluded from study entry because efficacy in this group has been established. In contrast to the previous studies, this study showed a significant increase in complications in the ERCP group compared with the conservatively managed group (respiratory failure, 12% versus 4% [P = .03]; renal failure, 7% versus 4% [P = .10]). In addition, the mortality rate was higher in the ERCP group compared with the control group (11% versus 6%), requiring premature termination of the study.56 The results of this large clinical trial suggest that in the absence of biliary obstruction or sepsis, ERCP may be harmful, and a conservative approach is preferred.
Oria and colleagues studied 102 patients with acute pancreatitis and an APACHE II score higher than 6; the subjects were randomized to receive ERCP within 72 hours or conservative management. Three patients in each group suffered local complications.57 Petrov and colleagues performed a meta-analysis of these trials.58 These authors concluded that the early use of ERCP did not significantly reduce the risk of local pancreatic complications in patients with either mild or severe pancreatitis.
In contrast, Dutch investigators reported their observational results of the use of ERCP as part of another clinical trial on the use of probiotics in SAP. Of the 153 patients enrolled, 81 underwent ERCP and 72 received conservative management. Of the 153 patients, 78 patients with cholestasis had fewer complications when ERCP was utilized [ OR 0.35; 95% CI, 0.13-0.99], but there was no significant effect on mortality, and no reduction of complications or mortality if cholestasis was not present in patients with predicted SAP.51 The role of ERCP in idiopathic pancreatitis also is unclear. Advances in ultrasonography and magnetic resonance cholangiopancreatography (MRCP) suggest that these modalities may have a preferred role when diagnostic considerations are the issue in acute pancreatitis, especially in view of the potential for complications with ERCP.59 As noted previously, endoscopic ultrasound may have an increasing role in identifying patients with suspected choledocholithiasis who might benefit from ERCP.
Magnetic Resonance Cholangiopancreatography
Magnetic resonance imaging (MRI) and MRCP are noninvasive imaging modalities that are useful for depicting abnormalities of the pancreatic duct and parenchyma.60–62 These imaging techniques can identify acute fluid collections and necrosis in SAP. MRI has several advantages over CT: there is no risk from radiation with MRI, it can detect pancreatic duct disruption, and it can help identify the etiology of acute pancreatitis. Without injection of gadolinium, MRI can discriminate between normal pancreatic parenchyma, the presence of edema, and the presence of necrosis as well as differentiate between solid and liquid fluid collections. In a study of 90 patients, 28 had gallstones, 9 had common bile duct stones, and 10 had pancreatic divisum.60,62 MRCP can be performed when ERCP has failed or is not possible, although ERCP is not only a diagnostic modality but also a therapeutic one, because the endoscopic approach permits sphincterotomy and removal of common duct stones.61
Contrast-enhanced CT is the gold standard for documenting pancreatic necrosis and assessing the severity of acute pancreatitis. Nevertheless, results from a few studies suggest that MRCP compares favorably with contrast-enhanced CT for the diagnosis and grading of severe acute pancreatitis.60,62 The major advantage of MRCP for SAP is that MRCP obviates the necessity for the infusion of iodinated contrast media and thereby may lower the risk for acute renal dysfunction in these critically ill patients.60,62 Bowel peristalsis, vascular motion artifacts, gastrointestinal air, and the presence of metallic clips all can degrade the quality of the images obtained with MRCP. One disadvantage of MRI and MRCP is that acquisition of the image takes longer than with CT.
 Management
Management
General Support
Monitoring and Resuscitation
Several publications suggest that patients with SAP should be managed in an ICU, preferably by a specialist team.17–1952 Ongoing monitoring for signs of distant organ dysfunction is crucial. Resuscitation of intravascular volume is a key component of the initial management, regardless of the etiology and severity of acute pancreatitis. Sequestration of fluid into the so-called third space (i.e., the extravascular extracellular compartment) can lead to loss of as much as a third of plasma volume. Rapid restoration and maintenance of intravascular volume is essential because hypovolemia and shock probably are important factors contributing to the high incidence of acute renal failure among patients with severe acute pancreatitis.30,63 It is common for patients with SAP to require administration of crystalloid fluid at rates as great as 500 mL/h, at least for a while.
Recently, 76 patients with SAP were randomly assigned to receive rapid infusion of IV fluid at either 10 to 15 mL/kg/h or 5 to 10 mL/kg/h, both groups receiving more than 10 L of fluid during their first 3 days of ICU care.64 The investigators in this study suggested that several outcomes were better in the group that received more gradual fluid expansion. The results of this trial are interesting but require confirmation before there is widespread adoption of the authors’ recommendations.
Single-organ or multiorgan dysfunction is common, and monitoring of respiratory status is essential. Respiratory and cardiovascular dysfunction are common and require prompt identification and supportive care. Adequate oxygen delivery to tissues and prevention of splanchnic ischemia are essential to prevent further organ injury. Vasoactive agents may be required, but they should be considered only after ensuring that intravascular volume has been repleted. In addition, because rapid administration of large volumes of IV fluid may be indicated, abdominal compartment syndrome should be considered and assessed.65
Even when systemic signs of adequate resuscitation are present, local inflammation in the pancreas can continue, leading to ongoing production of cytotoxic mediators. Accordingly, investigators have been interested in targeting this aspect of the disease process. Treatment with protease inhibitors has been successful in experimental models of acute pancreatitis and is used via continuous arterial infusion in Japan.63,68 A trial was carried out that compared no infusion with continuous regional arterial infusion of the protease inhibitor, gabexate mesilate, plus antibiotics.66 Treatment with gabexate mesilate shortened the duration of abdominal pain, duration of SIRS, and decreased the length of hospital stay. Circulating levels of several markers of inflammation also were decreased with the protease inhibitor.66 A national survey of clinicians in Japan indicated the following: severe pain disappeared after a short period of time of infusion of a protease inhibitor; infected necrosis was less common when both a protease inhibitor and antibiotic infusion were infused; and mortality was lower when continuous arterial infusion was initiated within 2 days.67
Although there has been significant interest in decreasing cytokine production by administering an anti-TNF antibody, this approach has not been shown to be beneficial in clinical trials, perhaps owing to the early peak of TNF in the disease process. Similarly, although administration of an IL-1 receptor antagonist has been beneficial in animal models of SAP, this approach has not yet been applied successfully in clinical practice. One of the more interesting potential therapeutic approaches is directed at decreasing calcium ion–dependent cytokine release by using administering a calcium channel antagonist. In one animal study, treatment with a calcium channel blocker use was associated with a dramatic reduction in TNF release and an associated improvement in survival from 40% to 80%.69 However, these data are experimental, and although of interest, both further experimental data and results from clinical trials would be needed before this strategy could be advocated for the care of patients with SAP.


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


