144 Acetaminophen, Aspirin, and NSAIDs
Acetaminophen
 Key Points
Key Points
• Acetaminophen (APAP) is available in numerous formulations, including cold, cough, and pain relief medications.
• ingestion of APAP is the most commonly reported exposure to a potentially toxic pharmacologic agent.
• APAP toxicity is clinically silent up to 24 hours after ingestion. If any abnormalities in vital signs or significant symptoms are present, a coingestant should be suspected.
• A blood specimen for serum APAP determination should be collected 4 hours after ingestion.
• The serum APAP result should be applied to the APAP nomogram for determination of the patient’s risk for toxicity.
• N-Acetylcysteine (NAC) is the antidote for APAP poisoning, and the approach to treatment depends on the timing of the ingestion and the serum APAP level.
• Oral NAC dosing consists of a loading dose of 140 mg/kg and maintenance dose of 70 mg/kg every 4 hours for 17 doses. An intravenous formulation of NAC is now approved for use and should be given when oral administration is not feasible.
• The serum APAP level should be measured in any patient with clinical suspicion of an overdose or an attempt at suicide or if a patient with an overdose exhibits altered mental status.
Presenting Signs and Symptoms
Table 144.1 summarizes the four stages of APAP poisoning. The clinical manifestations of an APAP overdose arise from the hepatotoxicity and resultant complications. Patients, even those who eventually progress to fulminant hepatic failure, are initially asymptomatic. Significant abnormalities in vital signs or clinical findings that become evident soon after ingestion should not be attributed to APAP alone; the emergency physician (EP) should pursue diagnosis and treatment of a coingested agent.
Table 144.1 Four Stages of Acetaminophen Poisoning
| Stage 1 (0-24 hr) | Asymptomatic | |
| Stage 2 (24-72 hr) | Onset of hepatotoxicity | |
| Stage 3 (72-96 hr) | Maximal hepatotoxicity | The patient exhibits clinical and laboratory manifestations of hepatic necrosis: varying degrees of hepatic encephalopathy, jaundice, renal failure, coagulation defects, and myocardial abnormalities. AST and ALT levels peak, the INR value rises, blood urea nitrogen and creatinine levels rise, and pH drops. Death may occur, typically 3-5 days after overdose. Death from fulminant hepatic failure may be characterized by cerebral edema, sepsis, multisystem organ failure, hemorrhage, and adult respiratory distress syndrome. |
| Stage 4 (4 days to 2 wk) | Recovery phase |
ALT, Alanine transaminase; AST, aspartate transaminase; INR, international normalized ratio.
Differential Diagnosis and Medical Decision Making
The objective of diagnostic testing after an overdose of APAP is to assist the clinician in determining which patients are at risk for hepatotoxicity and thus require further treatment. Laboratory evaluation is essential for all patients with potential risk because of the lack of reliable clinical manifestations early after APAP ingestion, when antidotal therapy is most effective. Risk is assessed through a thorough history and physical examination, as well as collection of a blood specimen for a serum APAP measurement 4 hours after ingestion—or as soon as possible in patients initially seen more than 4 hours after ingestion—and application of the result to the acetaminophen nomogram (Fig. 144-1). For patients who are seen late after ingestion and already exhibit signs and symptoms of hepatotoxicity or for whom the time of ingestion cannot be readily established, the serum aspartate transaminase (AST) level should also be measured. See Figures 144.2 and 144.3 for guidelines to assess risk after acute and chronic APAP ingestion. Acute ingestion is defined as a single ingestion occurring over a single period shorter than 4 hours.
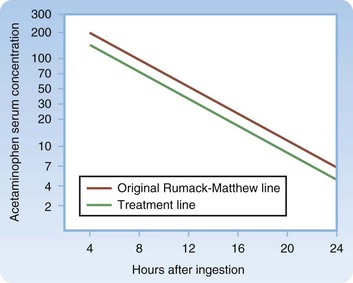
Fig. 144.1 Treatment nomogram for acute acetaminophen overdose.
(From Marx JA, Hockberger RS, Walls RM, editors. Rosen’s emergency medicine: concepts and clinical practice. 6th ed. Philadelphia: Mosby; 2006.)
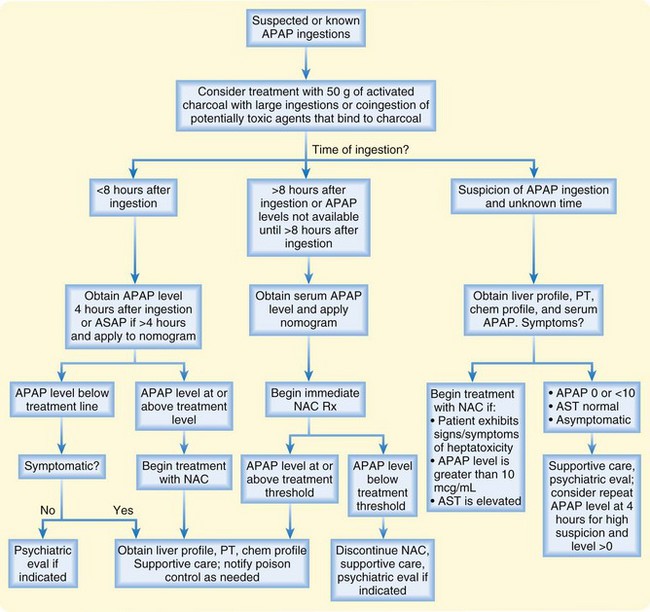
Fig. 144.2 Risk assessment and management of acute acetaminophen (APAP) poisoning.
AST, Aspartate aminotransferase; NAC, N-acetylcysteine; PT, prothrombin time.
If there is any clinical suspicion of an overdose, even if the patient does not admit to APAP ingestion or if the patient with an overdose exhibits altered mental status, the serum APAP level should be measured.1 Approximately 1 in 500 patients who have taken an overdose but do not admit to ingestion of APAP have a potentially hepatotoxic serum APAP concentration.
Treatment
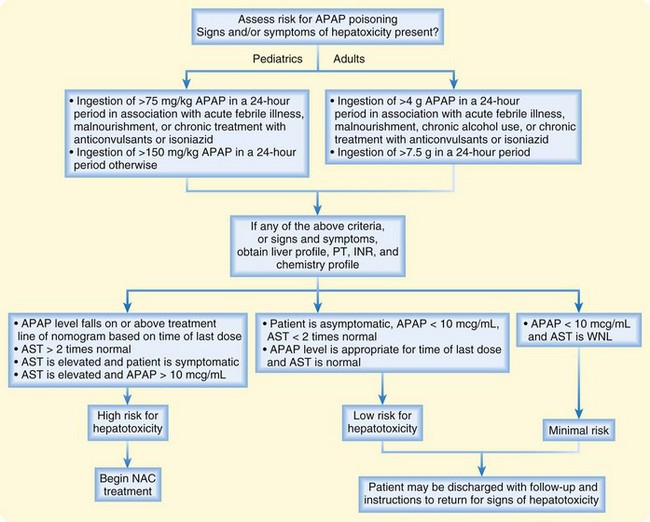
Treatment with 50 g of activated charcoal should be considered in patients with large ingestions of APAP or coingestion of APAP and potentially toxic agents that bind to charcoal.2 N-Acetylcysteine (NAC) is the antidote for APAP toxicity.3 If given within 8 hours of ingestion, the risk for significant hepatotoxicity secondary to APAP toxicity is low. There does not appear to be a significant advantage to administering NAC within the first 2 or 3 hours after ingestion over giving it later as long as it is within the 8-hour window. See Figures 144.2 and 144.3 for guidelines in determining which patients should be given NAC after acute and chronic APAP ingestion and in managing patient care. NAC is available in both oral and intravenous formulations.4 In general, both formulations are highly effective and well tolerated. Whether one formulation is superior remains controversial. See Box 144.1 for a comparison of the two formulations and Box 144.2 for dosing regimens.
Box 144.2 Dosing Schedule for N-Acetylcysteine (NAC)
Intravenous
Pediatric (<40 kg)
For patients weighing more than 10 kg, follow the package insert or regimen below
For infants less than 10 kg, dilute IV NAC to a 2% solution and then follow the dosing regimen below: Remove 50 mL from a 500-mL bag of D5W, and add 50 mL IV NAC (20%) to 450 mL D5W to create a 2% solution
Loading dose: 7.5 mL/kg (150 mg/kg) of a 2% solution over a 1-hour period
Second dose: 2.5 mL/kg (50 mg/kg) of a 2% solution over a 4-hour period
Third dose: 5 mL/kg (100 mg/kg) of a 2% solution over a 16-hour period




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


