Fig. 34.1
Classification of ventral hernias between the two lateral margins of rectus muscles. Five zones are defined. (Reprinted with permission from Muysoms FE, Miserez M, Berrevoet F et al. Classification of primary and incisional abdominal wall hernias. Hernia. 2009;13(4):407–414)
Fig. 34.2
For lateral hernias, 4 zones lateral to the rectus sheath are defined. (Reprinted with permission from Muysoms FE, Miserez M, Berrevoet F, et al. Classification of primary and incisional abdominal wall hernias. Hernia. 2009;13:407–414)
Table 34.1
Abdominal wall hernia operations in the USA during 1996
Type of hernia | Number of outpatient procedures | Number of inpatient procedures | Total number of procedures |
|---|---|---|---|
Inguinal hernia | |||
Unilateral repair | 458,000 | 62,000 | 520,000 |
Bilateral repair | 73,000 (76,000a) | 15,000 (30,000a) | 176,000a |
Total repairs | 604,000a | 92,000a | 696,000a |
Femoral hernia | 19,000 | 6,000 | 25,000 |
Umbilical hernia | 120,000 | 46,000 | 166,000 |
Incisional hernia | 40,000 | 57,000 | 97,000 |
Other abdominal wall hernias (epigastric, Spigelian) | 45,000 | 31,000 | 76,000 |
Table 34.2
The age and gender of herniorrhaphy patients in the United States during 1996
Gender (%) | Age (%) | |||||
|---|---|---|---|---|---|---|
Type of hernia | Male | Female | <15 years | 15–44 years | 45–64 years | >65 years |
Inguinal hernia | 90 | 10 | 18 | 29 | 23 | 30 |
Femoral hernia | 30 | 70 | <1 | 19 | 29 | 48 |
Umbilical hernia | 57 | 33 | 13 | 33 | 36 | 17 |
Incisional hernia | 35 | 65 | <1 | 25 | 35 | 39 |
Other abdominal wall hernias (epigastric, Spigelian, etc.) | 43 | 57 | 1 | 32 | 40 | 25 |
Groin Hernia Epidemiology
Groin hernias are divided into inguinal and femoral types. Inguinal hernias are subdivided into direct and indirect based on the relation of herniation to that of the epigastric vessels. Indirect hernias are lateral to the epigastric vessels and are generally related to a congenital weakness via a patent processus vaginalis. Direct hernias are medial to the epigastric vessels and bound by Hesselbach’s triangle, whose lateral border is the epigastric artery, the medial border is the lateral aspect of the rectus muscle, and the inferior border is the inguinal ligament. A Pantaloon hernia is an inguinal hernia with its sac extending through both the direct and indirect spaces. Numerous eponyms for femoral hernias exist based on anatomic location, such as Cooper’s (a hernia with extension into the femoral space and a second sac anterior to the femoral vessels), Hesselbach’s (hernia medial to the femoral vessels), Velpeau’s (hernia anterior to the femoral vessels), Serafini’s (hernia posterior to the femoral vessels), Laugier’s (hernia through the lacunar ligament), and Cloquet’s (hernia through the pectineal fascia). There are also eponyms based on what is contained in the hernia sac, i.e., Amyand’s (appendicitis in inguinal hernia sac), De Garengeot’s (appendicitis in femoral hernia sac), and Busse’s (testicle in hernia sac). The term “sliding hernia” when referring to a groin hernia is one in which a wall of hernia sac is composed of an organ, such as the bladder or colon. Finally, Gilmore’s groin, AKA sportsman’s hernia, is understood to be groin pain associated with dilated external ring and/or tears in the musculature or tendonous insertions in the area of the inguinal canal. Approximately 96% of groin hernias are inguinal and 4% are femoral. The overall lifetime risk of developing an inguinal hernia is 27% for men and 3% for women [14]. There is a 9:1 male-to-female predominance for inguinal hernias and a 7:3 female-to-male predominance for femoral hernias [2]. Groin hernia classification is important for purposes of literature review and comparison of techniques. As with most classification systems, numerous have been developed. However, the traditional classification of indirect, direct, and femoral remains the most consistent over time. In such, the most commonly used classification systems utilize these basic anatomic descriptors as seen in Table 34.3 [15, 16]. In 2002, the “Updated Traditional Classification” was proposed at a consensus conference and serves as the current method most commonly agreed upon today [16].
Table 34.3
Comparison of groin hernia classifications schemes
Traditional updated | Gilbert | Nyhus | Schumpelick |
|---|---|---|---|
Indirect | |||
1. Small | 1. Snug | I. Indirect, small normal internal ring, sac in canal | L1 < 1.5 cm |
2. Medium | 2. Moderately dilated ring | II. Indirect, medium enlarged internal ring, sac not in scrotum | L2 1.5–3 cm |
3. Large | 3. Greater than 2 finger-breadths | III. B. Combined–indirect large, encroaching into direct floor | L3 > 3 cm |
Direct | |||
4. Small | 4. Diverticular | III. A. Direct–Floor only. No more than one finger-breadth | M1 < 1.5 cm |
5. Medium | – | III. A. | M2 1.5–3 cm |
6. Large | 5. Entire floor | – | M3 > 3 cm |
Combined | |||
7. Pantaloon | 6. Combined | III. B. | Mc |
Femoral | |||
8. Femoral | 7. Femoral | III. C. Femoral | F |
0. Other | – | – | – |
Recurrent | – | IV. Recurrent A.Direct B.Indirect C.Femoral D.Combinations of A-B-C | – |
Clinical Presentation, Diagnosis, and Therapeutic Options
The acute care surgeon will encounter all types of abdominal wall hernias. Fortunately, there is little dilemma in the diagnosis of most abdominal wall hernias. As with any problem in surgery, careful history and physical examination will provide most all of what is needed to make the diagnosis. However, the diagnoses of some hernias, such as sportsman’s, Spigelian, femoral, and lumbar hernias can be challenging. The “sportsman’s hernia” incidence remains unclear, and its diagnosis relies almost completely on history and symptoms alone. Spigelian hernias only constitute 0.12% of all hernias [17], femoral hernias make up 2–8%[18] of all groin hernias, and lumbar hernias are so rare that it is likely most general surgeons will only have the opportunity to repair one in his/her lifetime [19]. Therefore, for these latter three hernias, the surgeon needs to have a high index of suspicion and employ judicious utilization of abdominal-pelvic computed tomography (CT) scanning to make a definitive diagnosis.
More often, the acute care surgeon will be faced with the emergent presentation of hernias with associated incarceration, obstruction, strangulation, and/or contamination, along with complex giant ventral hernias related to catastrophic loss of abdominal wall integrity. As such, this chapter will focus on the diagnosis and management of these two issues. Of note, although an important tool, even in the emergency setting, laparoscopic repair is not discussed in this chapter. One of the pitfalls we have encountered in this age of hernia repair is that many surgeons entering practice have performed very few “tissue-only repairs” (repairs without some type of mesh). This is especially salient when faced with the need to perform groin herniorrhaphy in a contaminated field.
Groin Hernias
The focus of groin hernia repair in this chapter has been limited to emergent tissue-only repair in a contaminated environment. In situations, where the surgeon encounters obstructed, strangulated bowel or perforated bowel, mesh placement is generally unfavorable. In these instances, the fundamentals of tissue-only repair remain immutable and the tenets of identifying bowel viability and control of contamination with bowel resection remain paramount. This is not to say that laparoscopic repair or mesh repair is absolutely contraindicated in emergency groin surgery; rather we have chosen to establish an updated reference of open tissue-only repairs for surgeons whose training may have focused on tension-free and laparoscopic mesh repairs. More than 70 tissue-only repairs have been described [20], with a handful remaining especially important for the acute care surgeon. Four tissue-only repairs provide an excellent foundation for groin hernia surgery in settings where the implantation of mesh is at high risk for infection. These are reviewed as follows.
Indirect and Direct Inguinal Hernia Tissue-Only Repairs
The Marcy repair is optimal for the small indirect hernias that are more often encountered in children and young adults. After dissecting the hernia sac free, the cord structures are retracted laterally and the hernia sac is ligated high. Subsequent approximation of the transverse aponeurotic arch to the iliopubic tract with one or two monofilament sutures (Fig. 34.3), returns the deep inguinal ring to its normal size, completing the repair.
Fig. 34.3
Marcy repair. (Reprinted with permission from Fitzgibbons RJ, Richards AT, Quinn TH. “Open Hernia Repair” in: ACS Surgery: Principles and Practice 2004. Wilmore DW et al. (eds) 603–624. WebMD Professional Publishing, 2004. In: ACS Surgery Online. Ed: Ashley SA. Decker Intellectual Properties (2012). http://www.acssurgery.com)
The Bassini technique is a three-layer repair that can be employed for any indirect, direct, or pantaloon groin hernias. The external abdominal oblique aponeurosis is divided along its fibers and the cord is identified and encircled. The cremasteric fibers are incised longitudinally. The medial flap is avascular and resected entirely, the lateral flap contains the genitofemoral nerve and spermatic vessels that can be divided and ligated. The indirect hernia sac (if present) can be ligated high or reduced. The surgeon then divides the transversalis fascia from the deep ring to the pubic tubercle and actualizes the preperitoneal space allowing for repair of the “triple layer” (transversalis fascia, transversus abdominis, and internal oblique muscle) (Fig. 34.4a). Nonabsorbable suture is used in an interrupted fashion to approximate the “triple layer” supero-medially to Poupart’s ligament infero-laterally. This begins at the pubic tubercle medially and ends with the recreation of a normal sized deep inguinal ring (Fig. 34.4b). If necessary, a relaxing incision can be performed medially to the internal abdominal oblique aponeurosis to reduce the tension prior to the repair.
Fig. 34.4
(a, b) Bassini repair. (Reprinted with permission from Bergman S, Feldman L, “Inguinal Hernia Repair” in: ACS Surgery: Principles and Practice, 6th Edition, Wilmore DW et al. (eds) BC Decker Inc, 2009. In: ACS Surgery Online. Ed: Ashley SA. Decker Intellectual Properties (2012). http://www.acssurgery.com)
The Shouldice repair [21] for indirect, direct, or pantaloon hernias incorporates the same initial steps as the Bassini repair. Following the opening of the transversalis fascia, a relaxing incision is created over the medial internal abdominal oblique aponeurosis. The repair uses two running nonabsorbable monofilament sutures (originally a 32- or 34-gauge steel wire), with the first starting at the pubic tubercle, approximating the iliopubic tract laterally to the undersurface of the transverse aponeurotic arch (transversalis fascia, transverses abdominis and internal abdominal oblique) (Fig. 34.5a). This moves supero-laterally to the deep ring, picking up the lateral stump of the cremasteric muscle to form the new deep ring, and returning back along the medial edge of the transverses and internal oblique to Poupart’s ligament, ending at the pubic tubercle and tied to itself (Fig. 34.5b). The second running suture begins at the internal ring grabbing the internal oblique and transversus muscles laterally and brings them to the external oblique aponeurosis just superficial to Poupart’s ligament. The direction is reversed and runs just superficial to itself, ending at the internal ring. Thus 4 suture lines are created in this repair.
Fig. 34.5
(a, b) Shouldice repair. (Reprinted with permission from Bergman S, Feldman L, “Inguinal Hernia Repair” in: ACS Surgery: Principles and Practice, 6th Edition, Wilmore DW, et al. (eds), BC Decker Inc, 2009. In: ACS Surgery Online. Ed: Ashley SA. Decker Intellectual Properties (2012). http://www.acssurgery.com)
Finally, the McVay repair is best suited for reconstruction of a femoral hernia with high risk for postoperative infection. Like Bassini and Shouldice, the initial steps of the dissection remain the same. After opening of the transversalis fascia and creating a relaxing incision medially, the repair is begun at the pubic tubercle with interrupted nonabsorbable monofilament suture. The transverse aponeurotic arch (lateral) is affixed to the deep and medial Cooper’s ligament (instead of the inguinal ligament as performed in the Bassini repair). This proceeds supero-laterally up to the medial and anterior femoral sheath, with a “transition stitch” into the inguinal ligament (Fig. 34.6). From here, the repair proceeds laterally as in the Bassini repair. Affixing the aponeurotic arch to Cooper’s ligament accomplishes the task of narrowing the femoral canal. Additionally, the complete repair fixes the deep ring, the myopectineal orifice and Hesselbach’s triangle. Thus, it addresses all areas of potential herniation.
Fig. 34.6
McVay repair. (Reprinted with permission from Bergman S, Feldman L, “Inguinal Hernia Repair” in: ACS Surgery: Principles and Practice, 6th Edition, Wilmore DW et al. (eds) BC Decker Inc, 2009. In: ACS Surgery Online. Ed: Ashley SA. Decker Intellectual Properties (2012). http://www.acssurgery.com)
Femoral Hernia Tissue-Only Repairs
Due to its low incidence and complexity, emergency femoral hernia repair remains a vexing problem in acute care surgery. They are the most common incarcerated groin hernia, and due to its higher incidence of bowel strangulation it carries a mortality of up to 14% [18]. Additionally, due to its multiple configurations (Fig. 34.7) [22], diagnosing its presence, choosing an optimal approach, and constructing an appropriate repair can be challenging. While the McVay repair is the mainstay for the inguinal approach to repair femoral along with any associated indirect or direct hernias, it is not a panacea. The acute care surgeon often faces tightly incarcerated, strangulated, or even grossly contaminated femoral hernias. The approach will be predicated on numerous factors, including size of hernia, the state of its contents, the ability to reduce the hernia and whether the diagnosis of femoral hernia was made preoperatively (versus misidentifying the hernia as inguinal preoperatively). Generally speaking, an inguinal incision 1 cm above the medial half of the inguinal ligament, will allow access to visualize the femoral hernia both above and below the inguinal canal [18]. In simple, non-contaminated cases with easy reduction of the bowel and sac, a repair can be accomplished by approximating the lacunar ligament to the pectineal ligament, thus closing the femoral space. In complex cases, when contents cannot be reduced but are viable, division of the lacunar ligament, from below the inguinal ligament, generally grants enough room to achieve reduction. The surgeon should ovoid dividing the inguinal ligament, as restoration of this structure is challenging at best.
Fig. 34.7
Variable locations of femoral hernias. (a) Hesselbach’s hernia. (b) Velpeau’s hernia (prevascular). (c) Femoral hernia. (d) Laugier’s hernia. (e) Serafini’s hernia (retrovascular). (f) Cloquet’s hernia. (Adapted from [22])
In cases where the contents are nonviable, the surgeon can proceed with two different approaches via the same incision. First, for large hernia defects, a trans-inguinal approach can be easily achieved. The transversalis fascia is opened and the neck of the strangulated bowel can isolated at its healthy point. Here the bowel is divided and a primary anastomosis can be performed. The necrotic bowel can be delivered distally from under the inguinal ligament and a McVay repair can be performed. Second, for smaller hernia defects, a preperitoneal approach can be achieved by developing a plane over the external oblique and then entering into the rectus sheath at the linea semilunaris. The rectus is retracted medially and the transversus is incised. The preperitoneal space can be developed toward the inguinal ligament. Here the neck of the hernia sac can be encountered. Again, the peritoneum can be opened and the bowel resected as above. After performing the primary anastomosis, the peritoneum is closed and a mesh-free repair can be achieved by approximating Cooper’s ligament to the iliopubic tract (Fig. 34.8) [23].
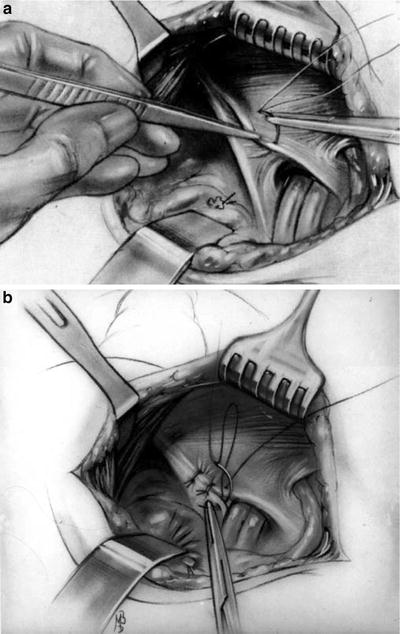
Fig. 34.8
Posterior preperitoneal approach to femoral hernia repair (Reprinted with permission from Nyhus LM. The posterior (preperitoneal) approach and iliopubic tract repair of inguinal and femoral hernias—an update. Hernia. 2003;7(2):63–67)
Complex Ventral Hernias in Acute Care Surgery
Complex ventral hernias constitute large (>10 cm diameter or 100 cm2) abdominal wall defects with a range of associate problems such as loss of abdominal domain, skin and soft tissue integrity deficiencies, enteric fistulas, and/or acute peritonitis with gross contamination. For 25 years, we contributed to the increase in complex abdominal wall problems through a practice of massive crystalloid resuscitation, thus promoting abdominal compartment syndrome with subsequent problems in the management of the open abdomen leading to fistulas and giant abdominal wall defects [24]. With the improving understanding of shock resuscitation, we might expect to see a decrease in the incidence of abdominal compartment syndrome and the need for the management of the open abdomen. However, on the flip side, patients may be more likely to survive from abdominal catastrophes due to improvements in surgical critical care, management of septic shock, and advancements in the care of complex enterocutaneous and “entero-atmospheric” fistulas. Three management strategies have evolved to address the repair of these complex problems. As it pertains to large defects (>10 cm), the first option is primary closure with bridging mesh. The second option is transfer of autologous tissue by rotational or free flap transfer with or without mesh reinforcement. Finally, the third option is components separation with or without mesh reinforcement.
The overarching theme for the approach to the management of ventral hernias is to restore abdominal wall integrity and dynamic function in a tension-free manner [4]. Five recommendations from the Ventral Hernia Working Group (VHWG) provide the evidence-based foundation for this goal (Table 34.4) [10, 25–32]. To accomplish this “meticulous attention to technique, timing, utilization of new technology, and tension-free repair in a clean, well-vascularized wound continue to be the cornerstones of the ideal repair” [33]. Therefore, performing a primary repair with bridging mesh is suboptimal, as restoration of dynamic function is not achieved. Reconstruction with rotational or free flaps is not desirable as they demand reduction of function and distortion of the donor site with poor functional results at the recipient site [34]. With this in mind, the utilization of components separation techniques (Fig. 34.9) pioneered by Donald H. Young in 1961 [35] and popularized by Oscar M Ramirez et al. in 1990 [36] has accelerated significantly in the past decade. Since 1990 there have been many modifications of the Ramirez components separation technique. In 1994 Fabian et al. [37] reported their modification with a more recent long-term follow-up report by DiCocco et al. that stated that their modification (Fig. 34.10) “…allows for more extensive mobilization and local advancement of autologous tissue, essentially doubling the mobilization compared with the original description” [38]. In the report by DiCocco, a variety of techniques were employed, including standard components separation (SCS) alone, modified components separation (MCS) alone, or SCS or MCS with prosthetic mesh implantation. They had a follow-up of 14.6 years (mean 5.3 years) of 114 patients with a 14% overall recurrence, but only a 5% recurrence when the MCS technique was employed without any prosthetic implantation. Interestingly, they had a fourfold increase in recurrence when a prosthetic mesh was used. This observation is disputed in other studies, which show that the addition of mesh reduces recurrence rates [27–29, 39–41].
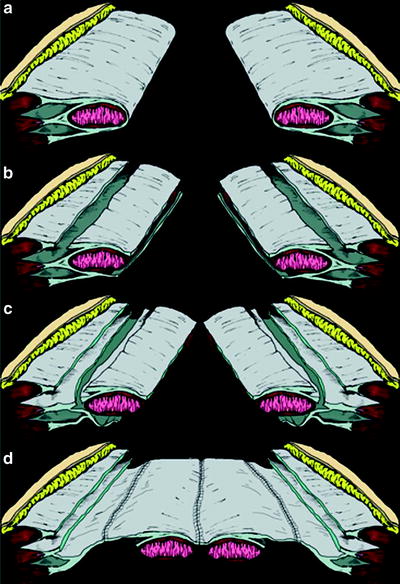
Table 34.4
Recommendations of the Ventral Hernia Working Group (VHWG) for the technique of repair of incisional ventral hernias
Recommendation | Strength of recommendation | Level of evidence | Evidence source (first author) |
|---|---|---|---|
1.Reinforcement recommended for repair of all incisional ventral hernias | 1 | A/B | Burger [26] Espinosa-de-los-Monteros [27] Luijendijk [10] |
2.Centralize and reapproximate rectus muscles when feasible under physiologic tension | 1 | C | de Vries Reilingh [28] Espinosa-de-los-Monteros [27] Kolker [29] VHWG opinion |
3.Reduce bioburden prior to repair | 1 | B | Mangram [30] VHWG opinion |
4.Placement of repair material: Underlay is the recommended technique for the placement of appropriate repair material for open and laparoscopic repairs; overlay placement of repair material should only be considered when complete fascia-to-fascia repair has been achieved | 2 | B | Awad [31] Espinosa-de-los-Monteros [27] Korenkov [32] VHWG opinion |
5.In the setting of gross, uncontrolled contamination, it is appropriate to consider delayed repair | 1 | C | VHWG opinion |
Fig. 34.9
Cross-sectional diagram of components separation. (Reprinted with permission from Ramirez OM, Ruas E, Dellon AL. “Components separation” method for closure of abdominal-wall defects: An anatomic and clinical study. Plast Reconstr Surg. 1990;86:519)
Fig. 34.10
Modified components separation technique for abdominal wall reconstruction. (a) Normal anatomy above the arcuate line. (b) The posterior rectus sheath is mobilized from the rectus muscle, and the external oblique fascia is divided. (c) The internal oblique component of the anterior rectus sheath is divided down to the arcuate line. (d) Completed repair, suturing the medial border of the posterior sheath to the lateral border of the anterior sheath, with approximation of the medial portion of the anterior sheath in the midline. Illustration by Steven P Goldberg. (Reprinted with permission from DiCocco JM, Magnotti LJ, Emmett KP, et al. Long-term follow-up of abdominal wall reconstruction after planned ventral hernia: a 15-year experience. J Am Coll Surg. 2010;210(5):686–695, 695–698)
There are no data to support or refute utilization of the components separation technique to achieve definitive abdominal closure in the face of acute illness associated with massive trauma or surgical sepsis. However, given recurrence and wound complication rates of 4–53% and 8–84%, respectively [25, 28, 33, 42, 43] for this technique, one should give strong consideration to winning the immediate battle and coming back later for the definitive closure procedure. A staged approach to the management of these complex problems has become accepted and may be necessary to reduce the risk catastrophic failures in order to increase overall long-term success [37, 42, 44–46]. In general, when faced with a patient who presents with multiple comorbidities in a high inflammatory state during the acute phase of trauma or sepsis, the surgeon should consider limiting the extent of the index abdominal closure to restoration of integrity only. Then, if necessary, the second stage can focus on restoration of both integrity and function, and can be delayed until such time as the patient recovers fully from their initial insult. The following three general scenarios utilizing components separation for repair of complex ventral hernias form the foundation of techniques that should be in the armamentarium of the acute care surgeon.
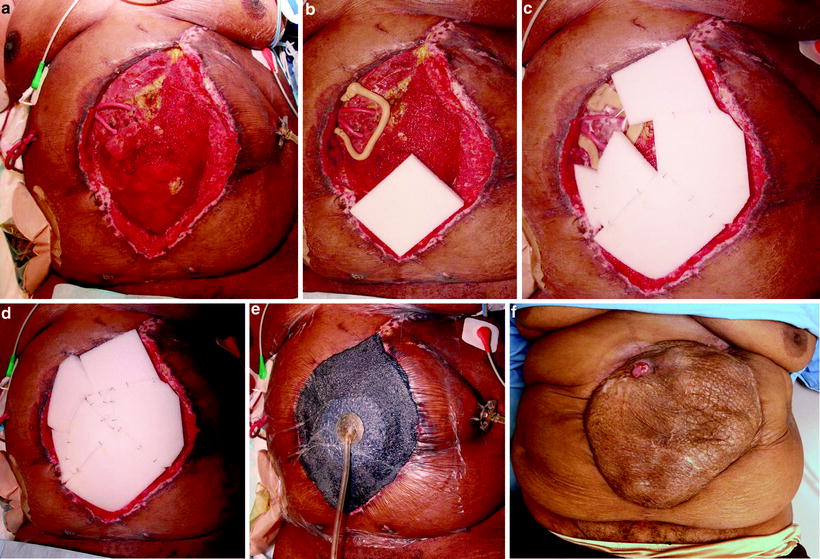
Scenario 1. Large Complex Ventral Hernia with Enterocutaneous Fistula
Enterocutaneous fistula(s) in the presence of a large ventral hernia can be safely managed as a single stage procedure [45, 47, 48]. Preoperative planning and preparation begin with local management of the fistula with special focus on protecting the skin from further damage and allowing for complete healing of the surrounding tissues. Attention must be paid to optimal nutritional support along with fluid and electrolyte control. For those patients who require total parenteral nutrition, optimizing wound care for rapid healing is critical, as these patients are at high risk for catheter related bacteremia and sepsis. The more complex “entero-atmospheric” fistulas will require massive time resources, attention to detail, extreme patience, and ingenuity (Fig. 34.11a–e). However, when taken care of well, the results can be truly amazing (Fig. 34.11f).