Fig. 27.1
Portrait of Bian Que. the earliest known physician of ancient China. (Courtesy of the Chinese Society of Anesthesiology, Beijing, China.)
Documents from the Eastern Han Dynasty(25CE-220CE) and the Three Kingdoms (220CE-265CE) periods indicate that Hua Tuo (Fig. 27.2) was respected for his expertise in surgery, anesthesia, and acupuncture, and that he was the first person in China to apply anesthesia for surgery. His general anesthetic combined wine with herbs in a concoction called mafeisan (“boiled cannabis powder”). The Book of Sui Dynasty listed five books attributed to Hua and his disciples, but none survived and Hua’s prescription for mafeisan has been lost [1]. Hua was also considered the first surgeon in China. He has been compared to Jivaka of India, who lived at the time of Buddha (about 500 BCE.) and was also renowned for surgery and anesthesia. Hua had no significant successors until modern times, when surgery and anesthesia were reintroduced by Western physicians [2]. Biographical information aboutHua Tuo appeared in English in three works: an article in theJournal of Traditional Chinese Medicine; [3] a monograph in Chen’sHistory of Chinese Medical Science; [4] and a report in theAdvanced Textbook on Traditional Chinese Medicine and Pharmacology [5].

Fig. 27.2
Portrait of Hua Tuo from a Qing Dynasty print. He was the first person in China to apply anesthesia for surgery. (Courtesy of the Chinese Society of Anesthesiology, Beijing, China.)
The Introduction of Western Anesthesia into China (1847–1949)
News of the 1846 public demonstration of ether anesthesia for surgery in the US [6,7] spread to London in December 1846 and Paris in January 1847. Peter Parker, who received degrees from both the divinity and medical schools at Yale, introduced ether anesthesia into China on 4 October 1847, using an apparatus received from Charles Jackson of Boston. He anesthetized a middle-aged farmer for the separation of the eyelid from the eyeball (symblepharon) in Canton Hospital, Guangzhou. A year later, Parker used chloroform in 8–10 cases, after reading a pamphlet written by James Simpson [8].
Anesthesia, as demonstrated by Morton and Simpson, was quickly introduced into large cities including Beijing, Tianjin, Shanghai, and Guangzhou. Open-drop ether or chloroform, along with local and spinal anesthesia were used throughout the rest of the 19th century and up to the middle of the 20th century. During this time, physicians, students, nurses, nuns, and technicians might administer anesthesia. Although the anesthesia methods were simple, gastrectomy, cholecystectomy, and even some neurological surgeries were successfully completed. For example, in September 1938, a pituitary adenoma resection was completed in the Peking Union Medical College Hospital (PUMCH) using a combination of local anesthesia with procaine and rectal anesthesia with Avertin.
Modern anesthesiology in China developed formally with the founding of Peking Union Medical College (PUMC) in 1921, by the US Rockefeller Foundation. FC Mclean, a 28-year-old graduate of the University of Chicago, and professor of internal medicine, was appointed the Dean. PB Seam was assigned as the president of its subsidiary hospital, PUMCH. General surgery, orthopedics, urology, gynecology, ENT and other surgical departments were immediately established. Miss Helen Holland was in charge of anesthetic delivery. From 1938 to 1941, Yueqing Ma, a 1934 graduate from PUMC, worked in the department of anesthesia as the first Chinese anesthesiologist in Beijing [Fig. 27.3]. The PUMCH was equipped with US-made equipment. A Heidbrink anesthesia machine and a McKesson intermittent flow anesthesia apparatus, believed to have been used in the 1940s, were found in the storeroom of PUMCH in the 1950s,

Fig. 27.3
Ma Yueqing, the first Chinese anesthesiologist in Beijing. (Courtesy of the author.)
Development of Anesthesiology in China (1949–1966)
World War II devastated China no less than Europe. The internal disruptions required to oppose the Japanese occupation were compounded by the Chinese civil war that followed. The Marshall Plan assisting reconstruction in Europe did not apply to China. Thus, anesthesiology, like all of Chinese medicine, faced enormous economic and physical burdens. Anesthesiology as a clinical specialty and science had to begin at ground level, starting in the great cities and spreading from there.
Pioneers in Chinese Anesthesiology
Before World War II, anesthesiology in China strove to keep pace with that in America and Europe. Interns and junior surgical residents were trained to administer anesthesia, but no formal residency program existed, nor was there a professional society to promote the “art and science” of anesthesiology. There was neither a Chinese textbook of anesthesiology, nor a journal devoted to anesthesia.
After World War II, the Ministry of Education underwrote grants to send promising physicians to North America for training in anesthesia with the hope that these physicians would return with the knowledge and expertise to ensure the growth of the specialty in China. The following includes brief biograhical sketches of some of these pioneers in Chinese anesthesiology.
Jone Wu
(Fig. 27.4), a 1938 graduate of the National Shanghai Medical College, had pursued a career as an instructor in pharmacology at his alma mater for almost a decade. In 1947, he won a Ministry of Education Scholarship to study anesthesiology in the US, and from 1947 until 1949, he studied at the University of Wisconsin in Madison. Wu returned to China in 1950, and founded the Department of Anesthesiology in Zhongshan Hospital of the National Shanghai Medical College, and established the first blood bank in China. By 1954, Wu founded an independent academic department of anesthesiology, to provide a clinical service to the six hospitals affiliated with the medical school. He also helped develop the first Chinese ventilator and anesthetic machine [9]. In 1954, Wu published the first Chinese-language anesthesia text, with a second, expanded edition appearing in 1959. He was instrumental in establishing postgraduate training in anesthesiology and personally trained more than 150 residents.
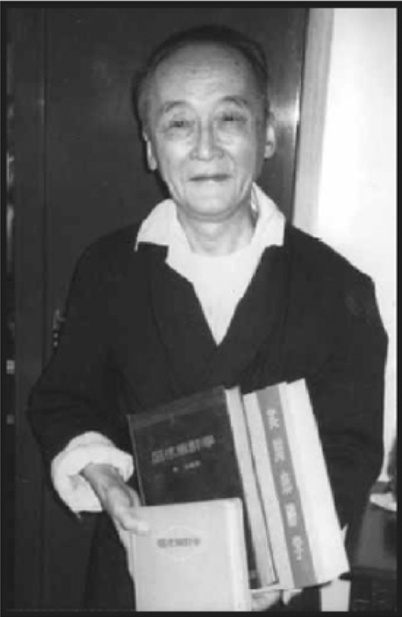
Fig. 27.4
A photograph of Jone Wu taken in February 1986 at his residence in Shanghai. He holds three books that he wrote on anesthesiology. The middle one is mentioned in the memorial tribute to him published in 1954 in Clinical Anesthesiology. (Courtesy of Joseph Rupreht, MD, PhD.)
Deyan Shang
(Fig. 27.5) completed a 5-yr medical program in Lanzhou University in 1942. After graduation, he served as a surgeon at his medical school, becoming chief resident surgeon in 1945. Because there was no anesthesia service in Lanzhou at that time, the chief executive officer of Lanzhou Central Hospital persuaded young surgeon Shang to pursue anesthesia training in America, and sent him to the anesthesiology residency program at the University of Illinois (Chicago) in 1948. Shang returned to China in 1949 and established the first Department of Anesthesiology in China in the National Lanzhou Hospital. He began a research program in cardiac physiology, critical care medicine, and resuscitation. In 1956, he moved from Lanzhou to the Fu Wai hospital in Bejing, a major teaching affiliate of the PUMC, where his career blossomed. In 1957, he established the first animal research laboratory in China, investigating issues associated with invasive cardiothoracic anesthetic management, hypothermic anesthesia for cardiac surgery, and resuscitative studies. Shang helped found the Chinese Society of Anesthesiologists (CSA) in 1979, and became its first president. In addition, he helped establish the Chinese Journal of Anesthesiology in 1981.
Fig. 27.5
Deyan Shang (1918–1985), the first president of Chinese Society of Anesthesiology. (Courtesy of the Chinese Society of Anesthesiology, Beijing, China.)
Rong Xie (Yung Shieh)
(Fig. 27.6) graduated from the Tong Ji University School of Medicine in 1946. He traveled to America, and received training at the Detroit Receiving Hospital in Michigan, affiliated with Wayne State University. He received additional training in Pittsburgh, Pennsylvania, before returning to China in 1950. He first traveled to his home province of Yunan to develop anesthesiology in the southwest region of China. In 1956, Xie started a collaborative relationship with Shang in Beijing. He was appointed associate professor at Peking Medical University in 1957, and succeeded Shang as the second president of the CSA, in 1984. He established the first Surgical Intensive Care Unit directed by an anesthesia department in China in 1985. He was also the founding editor-in-chief of the Chinese Journal of Anesthesiology.

Fig. 27.6
Rong Xie (Yung Shieh), the second president of the CSA in 1984. He established the first SICU directed by an anesthesia department in China in 1985. He was also the founding editor-in-chief of theChinese Journal of Anesthesiology. (Courtesy of the Chinese Society of Anesthesiology, Beijing, China.)
Xingfang Li
went to the US in 1947 for training in anesthesia. After returning to China in 1947, Li began work in the Renji Hospital at the Shanghai Second Medical School, establishing the Department of Anesthesiology there in 1954. Three years later, Li moved to the Ruijin Hospital, also affiliated with the Shanghai Second Medical School, where she established another Department of Anesthesiology following the anesthesia group established by the famous surgeon, Jixiang Shi. Li was an expert in hypothermia and cardiac anesthesia.
Huiying Tan
graduated from Yunnan Medical School, and went to Europe in 1947, to study and work in the Department of Anesthesiology of the University of Paris. In 1956, she returned from France and pioneered “artificial hibernation therapy”, a state of deep sedation induced with pethidine and chlorpromazine (or promethazine).
These five pioneers are credited with elevating the national standard of anesthesia in clinical training, research, and education. They were instrumental in shaping Chinese anesthesia.
Progress in Anesthesia Methods and Machines
In the 1950s, most anesthesia practice consisted of open-drop ether inhalation, local infiltration anesthesia, and single-injection spinal anesthesia. Some anesthesia machines were in use, and nearly all equipment was imported, including Heidbrink machines from the US, Drager machines from Germany, and Boyle machines from the British Oxygen Company. Meanwhile, domestic manufacturers progressed from simple imitation of non-Chinese equipment to modification and improvement of machines built in China. Chinese brands included the Shanghai Tao Gen Ji (later the “Zhong Hua” brand, similar to the Heidbrink anesthesia machine); the Zhonghua compound anesthesia machine (with an attachment for pediatric anesthesia), a multi-functional anesthesia machine (with positive and negative pressure ventilation), and the “103” closed circuit anesthesia machine. The first continuous-flow anesthetic machine was made in Shanghai in 1956, and the first artificial heart-lung machine was constructed, also in Shanghai, in 1957.
Most hospitals once used and are still using these products which combined quality and reasonable price. Chinese anesthesiologists were innovative and adaptive. If equipment was not ready-made, anesthesiologists used considerable ingenuity. For example, they might obtain smooth and slippery rubber tubing of appropriate diameter from grocery stores, and cut them into different lengths to make tracheal tubes. The distal end might be beveled and smoothed with sandpaper [10]. Meanwhile, other equipment was manufactured, including epidural and spinal needles, and laryngoscopes.
Related posts:
 History Reflected in the Evolving Approaches to Anesthesia for a Patient Undergoing Cholecystectomy
A History of Intravenous Anesthesia
History Reflected in the Evolving Approaches to Anesthesia for a Patient Undergoing Cholecystectomy
A History of Intravenous Anesthesia
 Major Anesthesia-Related Events in the 2000s and Beyond
Major Anesthesia-Related Events in the 2000s and Beyond
 1846–1860: Following the Discovery of Anesthesia
1846–1860: Following the Discovery of Anesthesia
 Major Anesthetic Themes in the 1960s
Major Anesthetic Themes in the 1960s
 The Evolution of Premedication
The Evolution of Premedication
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


